
Blood sugar basics- Insulin resistance – Blood sugar targets – Eating in hospital – Different carb counting methods – Foot care – What diabetics need to know
Blood sugar basics
Often you may notice that the blood sugar in the morning is higher than when you went to bed at night even when you have not had any bedtime snack. This can be due to a variety of causes including gluconeogenesis, the dawn phenomenon and delayed stomach emptying which is also known as gastroparesis. There are many other variables that affect blood sugar besides just the macro nutrients of the food you eat.
Gluconeogenesis
Gluconeogenesis (Latin for “the making of new sugar”) is the process where the liver converts protein to glucose. This goes on all the time to some extent but is suppressed in the presence of adequate amounts of insulin and drinking alcohol. In type one patients who are no longer able to make enough of their own insulin this process accelerates and is what causes their sugars to rise so high and for them to lose so much weight.
Dawn Phenomenon
The Dawn phenomenon is called this because the liver clears away insulin more efficiently first thing in the morning compared to other times of the day. At the same time growth hormones and sex hormones are manufactured during the night and these make cells less sensitive to the action of insulin which normally moves sugar from the blood into the cells. These two mechanisms result in higher blood sugars in the morning for most people after puberty gets underway. Various dietary and insulin techniques can be used to minimise the effects of this phenomenon.
Delayed Stomach Emptying / Gastroparesis
Delayed Stomach Emptying is due to the effects of long term nerve damage on the way the stomach works. The rate of stomach emptying is reduced and the bottom end of the stomach called the pylorus can go into spasm. It can be difficult to know how your stomach will respond from one meal to the next.
For type two diabetics who are not on insulin or drugs which stimulate insulin secretion this may simply give you very unpleasant indigestion.
For insulin users and those on drugs that stimulate insulin secretion, these are usually timed to act over the time the food of the meal is getting digested. When food digestion becomes imbalanced, blood sugars can be too low immediately after a meal only to go too high some hours later.
Special dietary measures are needed to overcome the effects of this condition and they are carefully explained in Dr Bernstein’s book Diabetes Solution.
Like many complications of diabetes it tends to become apparent after 5-20 years of diabetes depending on the level of blood sugar control. Although the condition can certainly make diabetes control much more difficult it is possible to reverse delayed gastric emptying and some other complications by careful maintenance of normal blood sugars for several years.
Genetic Factors
Blood sugars can rise over the long term from effects you can’t control like inheritance. Excess weight has both genetic and environmental components from the womb onwards. Excess weight gain raises your blood sugars because it makes you more insulin resistant.
Infections
Undiagnosed and untreated infections particularly gum and dental infections can raise your blood sugar. Careful examination by a dentist is often needed. Treatment can take months.
Acute Illnesses
Dehydration and acute infections such as gastroenteritis, viral infections, acute injuries, surgical operations or stress can raise blood sugars.
An important consideration is that once the blood sugar is high you become more insulin resistant because of this and vicious circles of high blood sugars, not being able to control them and dehydration can occur. This topic is further explored in the section on sick days in the insulin users section.
Chinese Restaurant Effect
The Chinese Restaurant effect named so by Dr Bernstein is the high blood sugars that rise disproportionately to the carb count of the meal due to the actual bulk of the meal. Moderate distention of the stomach produces the stimulation of the hormone glucagon which acts in opposition to insulin. This makes the liver produce more sugar from protein. The main thing to remember is not to stuff yourself at meals.
Exercise
Exercise affects blood sugars considerably. Different sorts of exercise can raise or lower your blood sugar. This also varies according to how much insulin you have working at the time. The factors are very complex and there will be more discussion and sources of information on this in the insulin users section of the course.
Exercise can improve many aspects of your life. Even if you have never been to a gym in your life and like me ran away from the ball at enforced school P.E. sessions there are so many activities you can enjoy. You can be active indoors, outdoors, in teams, alone, with help from instructors or by self discovery. Your mood, physique, strength, stamina and flexibility can all benefit in some way.
Insulin Effectiveness
Tainting a bottle of insulin or exposing it to extreme temperatures can both cause it to lose some of its effectiveness and hence will increase one’s blood sugar even though the same dosage is administered.
Quick Quiz:
![]()
What is true?
- The dawn phenomenon affects teenagers and…
a Makes their blood sugars particularly high when they wake up in the mornings.
b Makes them sleepy and unable to get up in the mornings.
c Makes their breakfast digest more slowly than usual.
d Makes their blood sugar high by releasing glucagon.Have you got it?
1. A is correct. The DP as it is often referred to also affects many adults.
Reference Info:
This section is based on the work of Dr. Bernstein’s Diabetes Solution.

This section is for all type twos and any type ones who think they are developing insulin resistance. This is often recognisable by an increasing waist line, blood pressure and need for high doses of insulin relative to your thinner years. Women with polycystic ovarian syndrome will benefit too.
When you eat carbohydrate it gets broken down by the digestive system and appears in the blood stream as glucose. Insulin is immediately released by the pancreatic beta cells. Insulin is the hormone that tells certain types of cell in the body to take up glucose in the bloodstream. In this way the glucose level in the blood stays within a narrow range.
In insulin resistant states such as metabolic syndrome and type 2 diabetes the cell wall insulin receptors are less sensitive to insulin and in an effort to keep blood sugar levels normal the pancreas releases more insulin.
High insulin levels causes inflammation and stiffening of the lining of your blood vessels. This lining is called the endothelium. This stiffening causes high blood pressure.
The pancreatic cells can initially make plenty of extra insulin to compensate for the weakened effect of the insulin but eventually become exhausted and start to die off. This causes higher blood sugars. Unfortunately blood sugars higher than 6.1 are toxic to beta cells and they start to die off with higher and higher blood sugars. The whole thing is a vicious circle.
Type two diabetes is often thought of as being less serious in some ways than type one diabetes. It is certainly true that a type two will not die as rapidly if they don’t get insulin as in type ones. On the long term however type two diabetes causes all the same complications as type one and can be just as fatal. Instead of it being obvious that something is drastically wrong with your health as in type one, those with type two can have it creep up on them over many years, slowly causing damage to the blood vessels, eyes, kidneys and nerves and not even know about it.
In type two diabetes there is initially more insulin produced to try to overcome the effect of insulin resistance. In early type two diabetes there can even be episodes of low blood sugars when the pancreas releases too much insulin at the wrong time. As time goes on the beta cells become exhausted and produce less and less insulin and die off. In many people insulin injections are eventually needed to give anything like normal blood sugar control.
Type two diabetics store less immediately available insulin than normal people. In addition they also need to produce more than normal because their cells are less sensitive to insulin. As their ability to produce insulin on demand declines they get higher blood sugars after eating and this persists for much longer than in non diabetic people.
High blood sugars after eating can be minimised by eating fats, protein and carbohydrates that release sugar gradually so that their pancreatic insulin factory (phase two insulin response) can keep up. This effectively means eating non starchy vegetables as the main source of carbohydrates.
For type two diabetics who do not need insulin they may get better results from eating 4 or 5 small meals a day rather than sticking to three bigger meals a day.
Many people have inherited their tendency to insulin resistance. If your parents or grandparents had heart disease, high blood pressure, fat round the middle, high cholesterol, high triglycerides, type two diabetes or swollen ankles you are more at risk.
The diabetes tendency becomes noticed at times such as pregnancy, ageing and if the person tends to eat a high sugar or starch diet. Lack of exercise also affects how rapidly the tendency will appear.
Insulin primarily affects blood sugar but also affects blood pressure, cholesterol and triglycerides and the storage of fat. No medications can reduce excess insulin production: only a low carb diet. A low carb diet works by reducing the over secretion of insulin and helps restore balance.
Beta blockers and diuretics which are often used to control blood pressure also increase insulin resistance and are best avoided in some people.
Although there are cut off points in blood sugar tests to say who is normal, who has metabolic syndrome and who has diabetes, the condition is really a continuum. Someone who has metabolic syndrome can get retinopathy, kidney disease and cardiovascular disease just the same as a diabetic.
The worse your sugar control is the worse your cardiovascular and complication risk. A popular test to do is the hba1c. This is the percentage of sugar attached to your red cells in the blood. Although a normal range of 4-6 is often given for instance it has been found that your risk goes up progressively from levels of just 5.0. It therefore makes sense to have as good blood sugar control as you can, particularly if you have a moderate to long life expectancy.
Tests that you can have done to find out your risk or severity of metabolic syndrome and type two diabetes include measuring your waist/hip ratio, hbaic, glucose tolerance test, fasting lipids and blood pressure.
There is a progression in how type two diabetes is treated:
Low carbohydrate diet
Appropriate weight loss
Exercise
Drugs that enhance insulin sensitivity or insulin action
Insulin injections with or without oral drugs.
People who have lived with high blood glucose levels for years can feel shaky or ill at normal blood sugar levels. They also can have blurred vision. A gradual adjustment of the target blood range and progressive reduction in carbohydrates can help these symptoms settle down.
![]()
Quick Quiz:
1. One of these is true for type two diabetics…
a They get less serious complications than type ones.
b They can have slowly developing damage to tissues without realising it.
c They need the same level of daily monitoring as insulin using type ones.
d Those not on insulin get on best with three meals a day.
Have you got it?
1. B is correct. Unfortunately the myth that type twos get less serious complications than type ones persists. Diabetes is certainly not as dramatic in onset as in type ones. Its insidious nature makes it harder to detect and so damage goes unchecked. It is the case that monitoring of blood sugars needs to be done a lot less often than in insulin dependants but dietary habits must be just as good. If reasonable amounts of a person’s own insulin are being made type two diabetics may have better sugar results with smaller and more frequent meals than the 3 or 4 a day advocated for type one diabetics.
Reference Info:
Most of the information in this section is from Dr. Bernstein’s Diabetes Solution: The Complete Guide to Achieving Normal Blood Sugars.
This section contains the core information on which your future health depends. It covers the essential points about monitoring your blood sugars for insulin users and type two diabetics.
The more normal your blood sugars are through the day and night and during and after meals the better able you are to prevent or delay complications.
“Eat to meter” is a shortened way to say that you eat whatever you like, whenever you like AS LONG AS YOUR BLOOD SUGARS STAY WITHIN THE NORMAL RANGE.
This is perfectly easy if you don’t have metabolic syndrome or diabetes but causes considerable difficulty for people with glucose metabolism problems.
Many diabetologists genuinely believe that diabetics cannot realistically achieve normal blood sugars. They hope that the best they can do is to monitor your inevitable decline in health that high blood sugars produce long term and sort out the worst of your complications with drugs, lasers and surgery.
There is no doubt that achieving normal blood sugars most of the time requires a lot of personal education, self experimentation, time and effort. Whether this is worth it or not is a decision that is only your own. It is after all your eyes, kidneys, feet and heart that are at risk.
Unfortunately the NHS and many other international health care systems do not currently provide an available, affordable and appropriate educational package to help you achieve normal blood sugars. Helping you get the degree of control you want is the purpose of this site. It is essential that you become an expert in your own type of diabetes and its management. This site has lots of ideas, book and internet based resources to help you. Joining a diabetes forum like the Dr Bernstein’s Diabetes Solution Forum or Diabetes Support UK can be a good way to get specific answers to your questions, get emotional support and encouragement and even make friends.
Before you start to change your diet or other management it is essential that you consult a doctor or diabetic specialist nurse so that any changes can be done in a planned, step wise and consistent way that will not have an adverse effect on your overall health. People on oral hypoglycaemic drugs and particularly insulin are likely to see a dramatic reduction in their dosage requirements and any change of diet will require close supervision and blood sugar monitoring so that dangerous and potentially fatal low blood sugars do not occur.
Normal fasting and between meal blood sugars for a fit young adult are 4.6. Blood sugars should not usually go below 3.5 even if a fit young person has not been eating or has been exercising vigorously. A healthy young person can expect to have a hba1c of less than 5.5 although the laboratory range takes the older and not so fit or slim population into consideration and often gives an upper limit of 6.0.
Pancreatic beta cells start to die off at blood sugar levels of only 6.1 and irreversible damage to nerve cells starts at sugar levels of 7.8 mmol/l The blood sugar levels we therefore recommend that you aim for are therefore:
Fasting or before a meal assuming 3 spaced meals a day:
Ideal: 4.6
Type Ones 5.0
or at least below 6.1
One hour after your meal has been finished a maximum blood sugar of 7.8
Two hours after your meal has been finished a maximum blood sugar of 6.5
In order to achieve these most people will have to go on a pretty strict low carb diet. As well as this you will need to understand about how other physiological events and exercise affect your blood sugars. Remember that you are making long term decisions about your health every time you eat. Very tight control may not be for everyone. Have a look at the next section which is applicable to type ones as well to decide what you are aiming for.
This section is summarised from Gary Schiener’s excellent book for insulin users, “Think Like a Pancreas.” and “Pumping Insulin” by John Walsh and Ruth Roberts.
Extremely tight control
Ideal for pregnant women or women who are planning a pregnancy. This reduces maternal and baby complications to almost non diabetic levels. In the USA some centres put these women on insulin pumps 9 months prior to a planned conception to help achieve this. Their blood sugar targets are much lower than in the UK. The use of continuous blood glucose monitoring devices are used to detect night time lows and warn of pump failure. A diet with no more than 40% calories from carbohydrate (which is still quite high) is given and high glycaemic foods are banned.
Hbaic target 4.8%
Premeals and bedtime 3.6-5.2
one hour after starting to eat 7.2
2am-6am 3.6-5.2
If these targets are not met the high or low blood sugars can cause damage to the mother and baby. A pregnancy may be lost. These targets are aimed to mimic what goes on in a non- diabetic pregnancy and the closer to target the less risk there is of damage. If permanent damage from high blood sugars can manifest itself and be crudely countable in the form of miscarriages, foetal deformity and birth complications after 9 months, what do you think goes on in your body over say ten years or more?
Unfortunately the will and infrastructure is not geared in the UK to offer this sort of support to pregnant women yet and in the USA it remains very expensive.
The plus point is that if you are willing to reduce your dietary carbohydrate sufficiently it is certainly possible to meet these targets and with less hypoglycaemia risk whether you are a type one or type two, male or female, pregnant or not, youthful or not so youthful.
Tight Control
For older children. They are going to have diabetes for a long time.
For those in honeymoon. This phase can be prolonged with tight control.
Experienced insulin pumpers. You have the technology to achieve this.
Low carbers. You will find it easier than most to achieve this.
hbaic is 5-6%
premeal target range 3.3-7.8
one hour post meal range less than 8.9
specific premeal target 5.6
The majority of the Bernies achieve this level of control according to a poll when this course was being set up. Of course some are at normal “non diabetic” blood sugar levels and others are much higher but working their way down gradually.
Typical Control
Ideal for drivers who wish to avoid hypoglycaemia.
Most adults.
New insulin pump users.
Whenever you are switching to a new insulin or delivery method.
hbaic range 6-7%
premeal target range 3.9-8.9
one hour post meal target less than 10
specific premeal target 6.7
These blood levels would have most diabetologists and endocrinologists cartwheeling down their hospital corridors with glee. These levels are great to get to when you have been struggling so hard with a high carb/low fat diet on insulin or perhaps are quite insulin resistant. Please be aware however that you will be delaying rather than preventing complications at these levels. I don’t want to take the wind out of anyone’s sails but when you have been low carbing for a while it does get progressively easier to hit these targets. If this is you do you think you could go a little lower?
Looser control
Ideal for babies and toddlers and young children whose food intake and activity is unpredictable. Youngsters also tend to me more mentally affected by recurrent or severe hypoglycaemia.
Adolescents may have great trouble keeping their levels other than this because of the great hormonal changes that are occurring. Control will become easier in your twenties so just do the best you can do.
Older diabetics and particularly those who live alone. Because diabetic complications develop slowly over several to many years you may be able to be more relaxed.
hbaic range 7-8%
premeal target 4.4-10
post one hour target 11
specific premeal target 7.8
To get good control you need to have the appropriate tools and help from your medical support team. You will need to test your blood sugars quite frequently and you will need to know something about carbohydrate counting.
Good records help a lot because you can see patterns in your control. Frequent high or low blood sugars at certain times of the day indicate that a change may be needed.
It is always best to sort out any low blood sugar problems first before you try to sort out the highs. Sort out baseline blood sugars before dealing with meal issues. Sort out problems that occur early in the day before tackling the problems that are going on later. More detailed advice on how to do this for insulin users is given in the type one section.
Keeping your diabetes in control is what enables you to enjoy your life and fulfil your other obligations. People who are consistent with their diet, avoiding unnecessary or frequent snacks tend to achieve much better blood sugar control.
Because you and your and the doctor will be making decisions based on your blood sugar levels you can improve accuracy by:
- Washing and drying your hands.2. Apply a sufficient amount of blood to the test strip (apply a sufficient amount of blood to the test strip at the first go–don’t “milk” the blood spot as this gives artificially high blood sugar readings).3. Code your meter accurately.4. Keep your meter with you or perhaps have one on your person and one in the house or car.5. Have a regular checking system so you don’t run out of batteries, strips or lancets.6. Record your findings at the time or before you go to bed for the night.7. Remember your record book when you visit the medical team or bring your downloads or meter with you.
- Do averages of several readings at the same times of the day to look for patterns in control. Between 3 to 14 days works well for many people depending on how stable your diabetes is and how many changes around exercise, meals and medications you are making.9. Patterns may vary with shift work, work or weekends, monthly cycles, weather conditions and seasons.10. Consider computer based logs that can produce graphs and charts to make this more visual and interesting.
![]()
Quite long Quiz:
1. Who is responsible for your diabetes management?
a I am responsible for my own diabetes management.
b The Consultant Diabetologist or Endocrinologist is responsible.
c The Diabetes Nurse.
d My family.
2. Three of these body parts are affected by long term high blood sugars. Which one is not?
a Heart.
b Eyes.
c Cartilage.
d Feet.
3. Damage to nerves starts at a blood sugar over which level? (The first number given is the UK, Canada and Australia measurements in mmol/l and the US figure follows. The US figure is the UK figure x 18)
a 4/72
b 8/144
c 12/216
d 16/88
- What foods cause a rapidly high blood sugar level?
a Starch such as bread and potatoes.
b Meat such as fish and burgers.
c Vegetables such as cauliflower and broccoli.
d Fat such as butter and cheese.5. Your hba1c test is …
a A test of whether you are anaemic or not.
b A test of your blood sugar over the last week.
c A test of your blood sugar over the last 2-3 months.
d A test of your blood sugar over the last year.6. A normal blood sugar after fasting and between meals is…
a 15/270
b 10/180
c 4.7/85
d 2.5/457. A normal blood sugar two hours after meals is…
a 20/360
b 10/180
c 8/144
d 6/1088. Your blood sugar is starting to be too low when it is..
a 1.9/35
b 2.9/52
c 3.9/70
d 4.9/889. A normal hbaic for a healthy non diabetic person is..
a 7.5%
b 6.5%
c 5.5%
d 4.5%Have you got it?
1. For most people taking this course the answer will be ME. If you are a child or have special needs eg visual problems you may need to rely more on your family.2. Cartilage is not affected by high blood sugars but other tissues certainly are.3. Levels of 8/144 or over are toxic to neurones. This is a frighteningly low level but did you know that pancreatic beta cells are affected adversely by levels of just 6.1/110 or over? - Starchy foods release sugar quickly. Mashed potatoes for instance release glucose faster than the table sugar some people put in their coffee. Not you of course!5. The hbaic test reflects the past 2-3 months blood sugars with a stronger emphasis in the last two weeks. High blood sugar spikes affect it more than low blood sugar dips.6. 4.7/85 is normal for healthy young people. This is why it is advisable for diabetics to aim for 4.7/85. Insulin users need to aim slightly higher at 5.0/90 to give a margin of error in order to avoid hypoglycaemia.7. D 6/108 and this can be lower for fit young folk. Many diabetic organisations give much higher targets ranging between 7.8/140 and 10/180. Gary Scheiner has found that 9 out of 10 USA kids had higher blood sugars than this when tested one hour after finishing their meals. These target levels may be considered as good as you can get for those on high carbohydrate diets but are not a reflection of what goes on in non diabetic healthy people. Normal blood sugars for diabetics is the aim of Dr Bernstein’s programme.8. 3.9/70 is getting too low. Below this you could be starting to be impaired for such things as driving. Most drivers wouldn’t realise they were impaired even at much lower sugar levels than this!9. A normal hbaic for a healthy young non diabetic person is 4.5%
Reference Info:
- This section’s information was developed from Dr Gary Shiener’s book, Think Like a Pancreas: A Practical Guide to Managing Diabetes with Insulin and some of his lectures that you can find on the presentations section of the children with diabetes website.
- What is Normal Glucose?
- Glucose Tolerance Test Reference Information
- I first came across the “Eat to Meter” concept from a post to another diabetes support forum

No matter how healthy you think you are, you never know when. In the next section we all need to get to grips with that most chilling of subjects, How To: Eat from a Hospital Menu. This is for everyone.
Ironically one of the most risky places for a diabetic to eat is as an inpatient in a hospital.
Because you are a diabetic you will be told by nursing and dietetic staff that you must choose from the “Healthy Eating” section of the menu. This “Healthy Eating” section is specifically designed to be high in carbs, lowish in protein and very low in fat. I’m not at all sure what kind of metabolism is suitable for this sort of diet but it it’s certainly not a good idea if you have the sort of metabolism that cannot handle sugar and starch. This is the situation for all those people with glucose intolerance or diabetes. Yes. You!
Cost cutting in hospital budgets has had effects at least in the UK. In a recent stay there was no protein source at breakfast at all. I brought in my own low carb cookies and fruit and tins of salmon.
It is necessary for you and your relatives to be very firm at the outset that you must be able to choose from the whole menu, be able to choose large or small portions as you desire and to bring in supplementary food items if necessary. This could include olive oil and vinegar to dress your salads, fresh temperate grown fruits, cheese, cooked meats, oatcakes and diet drinks.
For breakfast ignore the toast and cereals and porridge and go for the cooked breakfast and eggs in a large portion. (If your hospital even provides this!) Supplement this with a small portion of fresh fruit. Grapefruit and mandarin orange segments are often offered on hospital menus but they are usually tinned and sweetened with sugar so are best avoided.
Instead of digestive biscuits as a midmorning and mid afternoon snack try some cheese and oatcake with butter. Many hospitals routinely offer diabetics snacks as this used to be necessary with twice daily insulin regimes. You may not really need a snack however. If you are hungry at a snack time you may not have eaten as much protein and fat as you really needed to at the previous meal. If you are insulin dependent you will need to have lucozade or gatorade or snacks available for low blood sugar treatment. A longer acting carb and some protein can work well provided you are not too low.
For lunch and dinner pick large portions of meat, fish, poultry, cheese and egg dishes with vegetables or salad. Ignore any potatoes, chips, rice, pasta or bread items. Avoid deep fried battered food if possible due to the high hydrogenated fat content and carb content of the batter.
Before bedtime toast and biscuits are about the only thing that is offered in hospital. These are likely to be too high glycaemic for you and cheese and cold meat or cheese and oatcakes usually work better to prevent a blood sugar spike or night time lows.
Despite the difficulties in getting fed properly in hospital it is well worth the effort to keep your sugars normal. Your infection rate is decreased and your recovery will be faster.
![]()
Quick Quiz:
1. Maintaining normal blood sugars by following a low carb diet in hospital results in three of these. What won’t happen?
a Less post- operative infection.
b More chance of surviving a life threatening illness.
c Faster discharge from hospital.
d Getting on the dietetic staff’s Christmas card list.
2. In hospital suitable breakfasts for a diabetic are…
a Whatever the nurse thinks looks good from the healthy eating section of the menu.
b Porridge, skimmed milk, fresh orange juice with cholesterol lowering margarine.
c Toast, butter, boiled eggs, tinned grapefruit and mandarin oranges.
d Bacon, scrambled eggs, tomato, half a grapefruit.
3. The most risky eating situation for a diabetic is…
a As an inpatient in hospital.
b As a passenger in an aeroplane.
c From a roadside snack shack.
d As a guest at a dinner party that includes Miss Marple, Hercule Poirot, Ellery Queen, Lord Peter Whimsey and Detective Columbo.
Have you got it?
1. ABC have been proven to result from good glycaemic control in hospital. Sadly D is something that is not as likely from low carbing in hospital. Well there is a first time for everything and sooner or later dieticians will come on board. If you are the first patient to get a card in these circumstances we MUST hear about it!
2. D is correct. The others are too high in sugar and starch. At least with option C you could eat the boiled eggs. Unfortunately the “Healthy Eating Menu in hospitals usually entails LOW FAT. The sugar content is usually high and the protein content is usually low. Most hospital dieticians and nurses will automatically dragoon you into choosing from this menu unless you make it very clear that you object.
3. These are all very risky eating situations. How do you choose between them? In hospitals and aeroplanes you have a very restricted choice of meal. Snack shacks may not be as hygienic as you would wish. And someone always get poisoned when these super sleuths are near. The only way to deal with these risky situations is to plan ahead and that often means bringing your own meal.
Reference Info:
Acknowledgements for this section to John Gibson the first of my patients who stood up to the dietetic staff in the hospital I work in. I am also grateful to hospital administrative staff who did their absolute best to bully me into backing down. I would never have believed what was necessary to secure a guarantee of freedom from the “Healthy Eating Plan.” To cut to the chase YOU MUST THREATEN TO SUE THEM.
This section is necessary for everyone to read at least once: Carb counting
When you understand the complexities of carb counting you need to ask yourself if you need to learn it or not.
If you are an insulin user who wants to eat higher carb meals even just sometimes you do have to learn and become highly proficient at this skill.
If you are not on insulin you may prefer to have a “done it for you” sort of diet such as Dr Annika’s, the Life without bread diet or coming later in the How To: Follow Dr. Bernstein’s Dietary Plan section.
If you are an insulin user who would prefer not to carb count you will still need to have some idea of what sorts of relative amounts of carb different foods have. Whether you choose Dr Annika’s, Life Without Bread or Dr Bernstein’s diet you are still going to have to cut your carbs gradually and be very consistent particularly in the run in phase when insulin doses are reducing. You need to give this carb counting a very good effort. When you are eventually stable on a low carb eating plan that suits you it is entirely possible to keep to doing what you know works and hardly carb count after that point.
There are several methods of carbohydrate counting that are commonly used.
These all have their pros and cons. You need equipment or information sources for some of them. No matter how accurate you try to be you are likely to end up with an approximation of the carb content. The more of these methods you become comfortable with the more versatility you will have under different circumstances. In all cases you need to make the best estimate you can and notice the results you get. What would you change next time if your post meal blood sugars are not within your particular target range? By giving it your best guess and then testing you can build up a profile of how your body, medication doses, and insulin can cope with that particular meal at that particular time of day.
HOW TO LOOK UP CARB LISTS.
Carb lists of food items can come from various sources. There are published books, web based resources and chain restaurants will often publish leaflets to give you an idea of the carb count or have the information on a web site.
One of the difficulties however is knowing what portion size they have actually measured. Sometimes a food is listed by the amount of carb in 100g which is a little over 3 ounces. Other times cups, tablespoons, handfuls or the number of items eg grapes are listed with carb count. The most accurate way is when you have a standardised and individually packaged portion.
The website resources section in the metabolic syndrome section has some carb counting sites to help you get started. In addition here is list from some fast food and other restaurants. To put these figures into context the Atkins diet ranges from 20-120g of carb a day.
Burger King
Whopper 48g
Cajun Chicken deli wrap 48g
Large fries 53g
Sachet ketchup 4g
Chocolate ice cream sundae 26g
McDonalds
Big Mac 44g
French fries regular 28g
BBQ dip 12g
Apple pie 27g
Regular vanilla milkshake 63g
Kentuky Fried Chicken
Original recipe chicken drumstick (one) 7g
Chicken fillet burger 36g
Corn 11g
Crispy strip (one) 6g
Pizza
One medium slice Italian pizza 27-38g
Portion of lasagne 63g
One slice of garlic bread 11g
Indian
One portion of boiled basmati rice 110g
Chicken tandoori 2g
Chicken korma 16g
Vegetable curry 15g
Beef curry 6g
Naan bread 80g
Canteen/Bar food
Baked potato 70g
Chicken pie for one 32g
Meat pie for one 33g
Shepherds pie for one 37g
Battered fish 21g
Sweet and sour pork 34g
Chips/Fries small 31g
Chips/Fries medium 50g
Chips/Fries Large 73g
HOW TO USE THE EXCHANGE METHOD OF CARB COUNTING
The exchange method of carb counting was used for many years. Diabetics and their carers were taught what quantity of a carbohydrate containing food amounted to 10g, 12g or 15g of carbohydrate. The Life Without Bread Diet which I have described in the Metabolic section uses a certain number of 12g carb portions a day.
In general this method can be more accurate than the list method. For instance a third of a cup of cooked rice is around 15g versus about 110g for your average Indian restaurant rice portion. It is still subject to some error of course.
The American Diabetes Association have come up with a rough quantity guide to help you. This is for a woman’s hand.
one clenched fistful = one cup
palms sized quantity = 3 oz
thumb tip = one teaspoon
handful = 1 or 2 oz of snackfood
whole thumb size = 1 oz
With all the inbuilt imprecision that this method of counting has you will always have to compare what you think you ate versus the results you got. When you do have such items as nutritional scales or relatively accurate portioned control amounts it is helpful to compare what they look like versus your usual portion size to improve your eyeballing accuracy.
American cup sizes are used throughout.
All of these portion sizes amount to about 15g of carbohydrate unless stated otherwise.
Easy Averages
1/2 cup beans
one small slice bread
1/2 cup cereal
one cup milk = 10g
1/2 cup cooked pasta
1/3 cup cooked rice
one large apple
5 small apricots
6 apricot halves in juice drained
one small banana
half a large banana
20 blackberries or blueberries
32 cherries
3 medium clementines or satsumas
3/4 cup fruit salad
one medium grapefruit
ten large grapes or 20 small grapes
2.5 kiwi fruit
3/4 of a medium mango
2 slices of melon
one large nectarine
one large orange
2 medium peaches
7 slices of canned peaches in juice drained
one medium pear
3 pear halves in juice drained
3 slices of pineapple
3 medium plums
4 dried prunes
1.5 tablespoons of raisins
1/2 cup raspberries
one tablespoon sultanas
One medium slice of bread 24g
one slice of french bread 1.5 cm in length
1.5 bridge rolls
1/2 medium sized roll
one slice currant or raisin bread
1/4 cup breadcrumbs
1/2 medium chapati
one toasted crumpet
1/2 currant bun
1/2 English muffin
2 small slices garlic bread
one medium hamburger bun 24g
one large hamburger bun 42g
1/2 hot cross bun
1/5 naan bread
1/2 sweet pancake 15cm diameter
2 large poppadoms
one pitta bread
one small scone
2 taco shells
1/2 corn or flour tortilla
For most breads a 30g serving has 15g of carb
2 tablespoons canned sweetcorn
one small corn on the cob
120g roast parsnips
1/2 cup frozen peas
1/2 small baked potato
one very small boiled potato
10 crisps
2 tablespoons mashed potato
For most vegetables
1/2 cooked = one cup raw = 5g carb
1 and a half cooked = 3 cups raw = 15g carb
1/2 cup of cornflakes, fruit and fibre or rice krispies
2 tablespoons muesli
1 cup puffed cereal
1/2 cup rolled oats made with water
one biscuit of weetabix
For most cereals a 20g serving has 15g of carb
Apple juice 150mls
drinking chocolate powder 20g
unsweetened grapefruit juce 180mls
Lucozade 85mls
unsweetened orange juice 170mls
unsweetened pineapple juice 150mls
soft drink 140mls
1/2 cooked barley
1/3 cup bulgar wheat
1 and a half teaspoons cornflour
1/3 cup couscous
2 and a half tablespoons wholewheat flour
2 tablespoons white flour
1/2 cup pasta
1/3 cup cooked rice
1 and a half tablespoons dried rice
1/2 cup tinned spaghetti
3 tablespoons baked beans
1/2 cup kidney beans
2 heaped tablespoons lentils or split peas
3/4 cup custard
3/4 cup evaporated milk
1 and a half cups milk
1/2 cup vanilla ice cream
2 heaped teaspoons sweetened yoghurt
1/2 standard bounty bar
25g bar of chocolate
1/3 standard mars bar
1.5 small milky way
1/2 snickers bar
3 fingers of kit kat
one finger of twix
3 cream crackers
3 crispbread
120g peanuts
3 cups cooked popcorn
25g packet of crisps
one penguin biscuit
two ginger nuts
one 9g shortbread biscuit
one 5cm square cake without icing
one 2.5 cm square cake with icing
one mr kipling french fancy 19g
one choc chip cookie 8g
one small slice chocolate cake
2/3 large croissant
one danish pastry
1/2 jam donut
1/2 slice fruit cake
one jaffa cake 9g
3 level teaspoons jam
one small slice madeira cake
1/2 an individual jam tart
1/2 mince pie
2 oatcakes
3 level teaspoons sugar
one small slice swiss roll
one small waffle
For most dry biscuits and cakes a 25-30g serving will have 15g of carb
For most sweets a 10-20g serving will have 15g of carb.
HOW TO COUNT CARBS USING CARB FACTORS
The carb factor is the percentage of carbohydrate present in a food. If an apple has a carb factor of 0.13 this means that 13% of the weight of that apple is carbohydrate. If your apple weighs exactly 100g this would contain 13g of carb.
To use this method you need a list of carb factors and a set of scales to measure out the weight of your food portion. Nutritional scales have the carb and other factors built into them but you can use any scale provided it is sensitive enough. Digital scales may therefore be preferable to analogue scales.
John Walsh and Ruth Roberts book, “Pumping Insulin” has a list of about 300 foods at the back.
The site Friends with Diabetes is a site for diabetics who wish to follow a kosher diet. There is lots of helpful information of help to everyone else too.
Also, this site www.medexplorer.com/nutrition/nutrition.dbm gives you carb content and other nutritional information too.
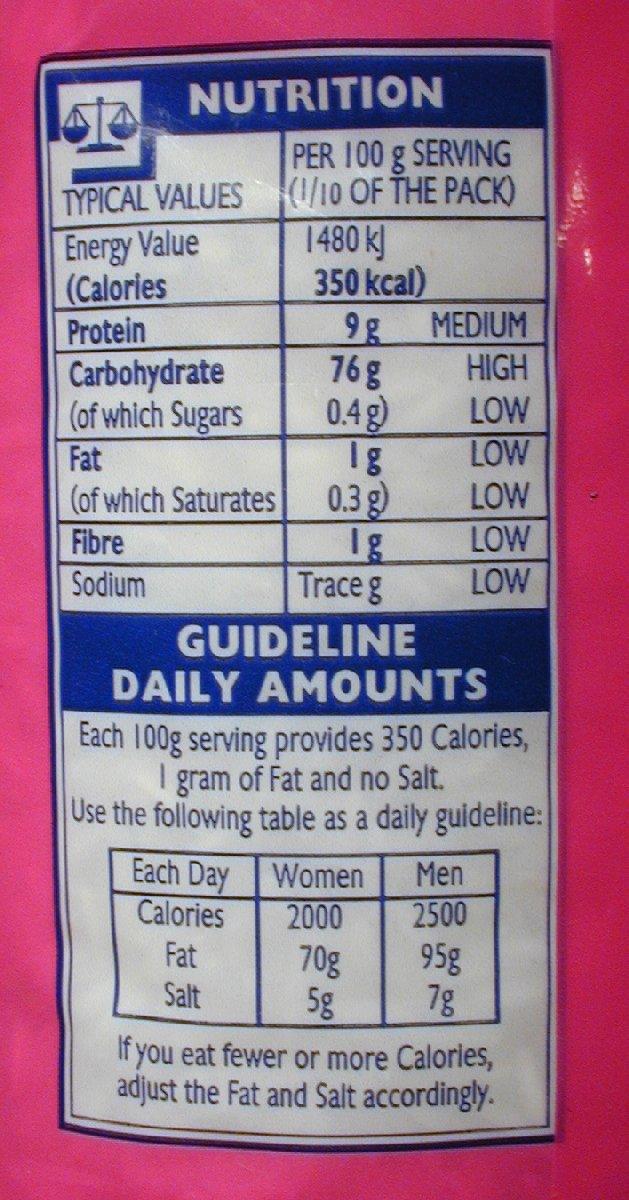
HOW TO COUNT CARBS FROM NUTRITIONAL LABELS
When you pick up many items of processed food you will find nutritional labels on them. How do you know how much carb is in the portion you intend to eat?
For the purposes of illustration let’s say I decide to have a meal of a half can of lobster bisque soup, 3/4 of a can of spaghetti bolognese and half a can of mandarin oranges in light syrup with a dollop of tinned heavy cream.
I look at the lobster bisque. It lists :
Per 100g
Energy 51 kcal
Protein 3.4g
Carbohydrate 4.7g
(of which sugars 1.2g
Fat 2.1g
(of which saturates 1.2g)
Fibre 0.2g
Sodium 0.5g
I want to eat half a can and fortunately the figures for this are listed too.
How to I know how much carb to count? In this case it is easy because it is on the tin. Carbohydrate 9.8g per half tin (of which sugars 3.5g).
The important thing to remember is that it is the carb count and not just the sugar count that matters.
Now for the main course. Tinned spaghetti bolognese. The tin weighs 400g.
I pick up this can and go straight to the carb count.
It says carbohydrate 13.2 per 100g with sugars being 2.4g of this.
Per half can serving there is 26.3g with sugars being 4.8g of this.
Ignoring the sugar content as usual I see that if I want 3/4 of the can I will need to do a little sum.
Although this is an easy sum to do I would like to go through what your old school teacher called “the working” so that it is easier to do this cross multiplication technique with more awkward amounts.
If 100g weight = 13.2 carbs what does 300g weight contain?
Write it like this 100g = 13.2
300g = X
Now cross multiply like this:
100g x X = 13.2 x 300g
From algebra you may remember that if you want to know what X is you need to move the 100g to the other side of the equal sign. When you do this it has to go below the 13.2 x 300g sum to indicate that this is now going to be divided.
So you get:
X = 13.2 x 300g
100
Using a calculator the answer is:
39.6
This cross multiplication technique can be used not only for counting how much carb is in a certain weight of food if you have the carb factor or carb count from a list but how much of a certain food you can have to stay within a certain carbohydrate limit.
Now dessert. Mandarin orange segments in light syrup. The can weighs 312g and the drained weight of the can is 170g.
Per 100g for the fruit and the syrup the carb count is 14g of which sugars is 14g.
For half a can the carb weight is 22g of which sugars is 22g. The fibre content is 1g.
This fibre content is pretty low so can be ignored in this calculation. For certain foods with a significant fibre level you may be best to deduct it from the total carb count. Fibre affects the bulkiness of the meal but as it passes through the gut without being absorbed you don’t need insulin to cover it. Because bulk can affect blood sugars through the effect of glucagon released from gut distention Dr Bernstein suggests a compromise by deducting half of the fibre from any given meal.
In this case we can find out how much carb is in half a can just by looking at the label. But what if this information was not supplied? What if the can contents had been shared out and you really had no idea what proportion of the can you had been given?
Let’s go back to the carb factor information. 14g of the weight of the 100g of this food is carbohydrate. If you weigh your portion on an accurate scale and it comes to 156g how much carb is this.
Cross multiply:
100g = 14g carb
156g = X carb
100 x X = 14 x 156
X = 14 x 156
100
X = 21.84g carb
Now let’s add the cream. Per 100g the carb count is 3.6g. For a 50g serving size the carb count is 1.8g. The can contains 283g so a serving size is 283/50 = 5.66th of the tin. A good couple of tablespoons by the look of this for a very low carb count.
Now add up your meal carb content:
Lobster bisque 9.8
Spaghetti bolognese 39.6
Mandarin oranges 22
Cream 1.8
Total = 73g
Now, you won’t be surprised to hear after what we’ve been telling you about high amounts of carbohydrate messing up your blood sugar control, weight and metabolism that this menu is for carb counting lessons only. You want to eat much healthier meals that this canned rubbish don’t you?
HOW TO COUNT CARBS USING NUTRITIONAL SCALES
Nutritional scales come in two main types. The cheaper type has a booklet with food lists and you enter the code of what you are weighing into the machine. More expensive models have an inbuilt computer with the foods listed and you click on the food you are weighing. These tend to have a larger database and can be used without having to have a booklet.
The nutritional scales give you the calorie, salt, protein, fat, cholesterol, fibre and carbohydrate counts for any given weight of food. There are memory features too.
The Salter nutritional scale that I have has 800 foods listed from the USDA database. It cost me £32 from Amazon. If you go onto the USDA site to find an even larger range of foods and have an accurate enough scale you do not really need to have nutritional scales. I have found it a convenient and useful method and our family even have guessing games about how many carbs a particular food portion contains. I have even taken it into restaurants to carb count food!
HOW TO EYEBALL PORTIONS OF CARB CONTAINING FOOD
Out of all the carb counting methods I have discussed this is the method subject to the most error and yet it is the most commonly used.
A book and its phone app Carbs&Cals&Protein&Fat by Chris Cheyette and Yello Balolia is very helpful for the general eater but is of limited help for the low carber. This is because much of the meals are of the canteen/ convenience variety that tend to be very high in carbohydrate.
To get success with the eyeballing technique you have to practice and practice with the other more accurate methods of weighing out small portions of food and using packaging information, charts or nutritional scales to come to what still is an approximation of the amount.
It has been shown that eyeballing is reasonably effective up to about 30g of carb portions but once the portions get bigger the estimates get considerably less accurate. For this reason you are better to look at your food and even move it about in your plate a bit try to replicate the portions you use at home with a known carb count and then add them up.
It always amazes me just how much carb potatoes have compared to for instance cauliflower, broccoli and green beans. Some eye ballings rules are that a golf ball size of mashed potato is 10g of carb and a woman’s fist size of cooked low starch vegetable is 5g.
The lower the carb count of your meal the easier it is in general to figure out the carbs. There is less room for error with what you think is one golf ball size of mash compared to say six such estimated portions which is not unusual in some restaurant meals. This goes of course for rice, bread, pasta, chips, cakes and sugary sauces too.
Partly for these reasons of difficulty in carb estimation and also because of the variability in the absorption and effect of insulin injections it is far less troublesome to simply keep these food items to a minimum for insulin users.
Type 2s who don’t use insulin also find that their sugars spike with anything other than modest portions of these items because they don’t have a supply of immediately releasable stored insulin in their pancreases.
![]()
Quick Quiz:
If you have been practising carb counting for a wide range of foods you can try this quiz. Carb counting is not an exact thing. Different breads are sliced to different widths for instance. Cup sizes vary too. In the carb comparison questions one option will have at least twice or half of the relative amounts of the other three options.
1. 12g of carbohydrate is present in all of these except…
a one thin slice of bread.
b one cup of broccoli.
c one cup of rice.
d half a grapefruit.
2. 15g is present in all of these except…
a Half a cup of beans.
b Half a cup of cereal.
c Half a medium roll.
d One hamburger bun.
3. 15g of carb is present in all of these except…
a One large banana.
b One medium pear.
c Three pear halves in juice.
d 3 medium satsumas.
4. 15g of carb is present in all of these except..
a Half of a small baked potato.
b A packet of crisps.
c A small portion of Burger King chips.
d Two tablespoons of mashed potato.
5. 15g of carb is present in all of these except…
a Three fingers of kit- kat.
b Half a standard bounty bar.
c One standard snickers bar.
d One finger of twix.
6. 30g of carb is present in all of these except…
a A slice of pizza (the size of the ones with a thin base served at the buffet in Pizza hut)
b A donut.
c Two oatcakes.
d An individual jam tart.
Have you got it?
1. C. A cup of rice is about 30g. More than twice the carb count of the others.
2. D. A small hamburger bun is around 24g and a large one 48g. The others are about half the carb count.
3. A. A large banana is about 30g.
4. C. A small portion of Burger King chips is about 32g. Even then the consistency between these small portions varies a lot. I know. I’ve sat counting chips to find out.
- C. A standard snickers bar is 34g.6. C. Two oatcakes at 7g each are around 15g.Reference Info:
Jo Sutton an Australian Dietician compiled the carb lists that I have used here.

This section is for all diabetics: Foot care.
You must treat your tootsies like little babies. You must be constantly vigilant that they are safe and warm but not too hot. You must call your doctor or podiatrist at any sign of anything that looks wrong.
Nerve damage to the feet due to the effects of high blood sugars takes between 5-20 years to become evident from diagnosis for most diabetics. Lack of sensation makes your feet more vulnerable from things that you may not even feel like tight shoes or a little gravel in the shoe. High blood sugars provide a nice growing medium for bacteria. Blood vessel damage to the area supplying the feet make injuries take much longer to heal in diabetics.
Dr Bernstein runs a specialist wound clinic for diabetics and has studied the causes of injury which have led to amputations. His book Diabetes Solution has a long list of dos and don’ts some of which you may know and others which you may not. I have not included every tip but would encourage you to buy the book and follow them.
Some tips are:
- Buy your shoes late in the day and make sure they do not pinch.
- Before putting on your shoes shake them out and make sure the linings are smooth.
- Have at least two pairs of shoes that you alternate every few days.
- Examine your feet for any injury or undue redness every day or get someone else to.
- Apply vegetable or animal oil every day to keep the skin soft eg olive or almond oil or emu oil.
- Don’t smoke.
- Keep your feet away from direct heat and avoid overly hot or prolonged baths.
- Wear warm socks when it is cold. Woollen are good.
- Avoid beta blockers if you have dry feet.
- Don’t file down or shave callouses or corns. These are nature’s way to protect you from abnormal pressure. Get appropriate insoles, padding or bigger shoes. A specialist podiatrist or biomechanical evaluation may be required for this.
- Get someone who can see what they are doing to trim your toenails if your vision is poor or not that flexible. Get a podiatrist to teach you how to care for your feet and nails.
- See an experienced nurse or doctor if you get any foot injury right away. It can be a disaster if infection gets hold. You may require high dose antibiotics, dressings and even hospital admission.
Ayrshire and Arran Health Board Podiatry Service have some additional information on foot care.
Washing your feet:
Wash feet every day but avoid keeping them in water for any longer than necessary.
If you intend to cut your toenails keep them in water for up to five minutes to let the nails soften.
Dry carefully between the toes.
If you have sweaty feet apply a light dusting of talc.
Footwear Advice:
Have your feet measured for length and width.
Everyday walking or working shoes should have:
Heels no higher than 3.5 cm or 1.5 inches.
Have lacing, buckles or velcro to hold the foot securely and prevent unnecessary movement.
The toe should be round or square.
Uppers should be made of a breathable material such as leather.
Soles should be thick and cushioning not thin and unyielding.
High heeled, pointed toe shoes, mules or strappy sandals are best avoided. If you want to wear them for a special event keep them to short periods. Don’t have sandals that have thongs between the toes.
Ensure your socks fit well. Change your socks once or twice a day and throw out any that are too small or which have holes. Don’t darn the darned things. Get rid of them!
Measuring your feet:
Your feet should be measured from the heel to the tip of your longest toe. For some people this is the second toe not the big toe. Congratulations if this is you. The Ancient Greeks regarded this as a sign of beauty!
You can check the length of your shoe by standing bare foot on a piece of thin cardboard and marking the place reached by the longest toe. Then place a thin strip of this into the shoe. There should be a one centimetre gap between the end of the cardboard and the heel of the shoe.
Your shoe width should match your foot width.
If you have a diabetic foot ulcer:
If your foot swells, changes colour or becomes more painful you must seek prompt medical attention. This means the out of hours or accident and emergency services if your doctor’s office is shut.
Podiatrists usually need to look at your feet very regularly and change dressings. You may be advised to shower or bathe less frequently and may need to stay off the foot more than usual. For some daily tasks you could be advised to sit instead of stand.
Healing will be more difficult if your blood sugar control is poor, you don’t rest the foot as advised, your footwear is not suitable, you forget to take medication as prescribed, you miss appointments, you interfere with dressings, or you continue to smoke.
Ulcers heal best when they are not taking your physical weight. Rest, elevation, special shoes, orthotic devices, crutches, zimmers, wheelchairs or plaster casts may be required at one time or another.
If you or a carer has been trained to do so, you may find that doing your own dressings is more convenient. A key component of this is knowing when and how you need help. There is always a risk that a serious foot infection can develop.
The most important factors in healing foot ulcers are achieving normal blood sugars and avoiding unnecessary pressure.
Antibiotics:
If you are prescribed antibiotics you must take them. For most diabetics the courses of treatment will involve several different antibiotics at much higher doses and for much longer than the equivalent infection in a fit non diabetic person.
One estimate is that it takes 50 times the amount of blood to heal a diabetic ulcer than a non diabetic ulcer.
Certain organisms found in probiotic drinks have been found to reduce the chances of getting diarrhea or diarrhea from a serious bacterial strain such as Clostridium difficle. The names of some of these probiotics are Lactobaccillus casei, L bulgaricus and Streptococcus thermophilus. Some commercially available yogurt drinks have probiotic organisms in them. It may be worth your while speaking to your doctor about taking such a preparation if you need a prolonged course of antibiotics. Remember to look out for any extra carbohydrate in the preparations. Sugar is often added to make them more palatable.
Typical antibiotic regimes:
Superficial ulcers:
Co-amoxiclav aka Augmentin 625mg three times a day.
or
Ciprofloxacin aka Ciproxin 500mg twice a day.
For 10-14 days.
Deep Ulcers
Clindamycin aka Dalacin 150 or 300mg four times a day.
and
Co-amoxiclav aka Augmentin 625mg three times a day.
and
Metronidazole aka Flagyl 400mg three times a day.
Duration of triple therapy depends on the severity of the ulcer but generally should be considered for six weeks.
Deep ulcer plus active cellulitis (skin infection):
Give the same sort of triple therapy regime but also add intravenous antibiotics. This could be Augmentin and Metronidazole. The choice of antibiotic is guided by the patient’s sensitivity and a medical microbiologist can help to choose the most effective regime.
For patients with penicillin allergy Erythromycin 500mg four times a day or Clarithromycin 500mg twice a day can be substituted.
A medical microbiologist will need to be consulted if the wound does not heal or there is active infection in the skin or bone.
Flucloxacillin is a typical penicillin which is used in non diabetics with soft tissue infections. In diabetic ulcers it simply cannot kill the range of bacteria that are likely to be present and so must not be used as a single agent.
Antibiotics can have nasty side effects such as diarrhea, stomach upsets, rashes, the growth of other pathogenic bacteria and liver and blood disturbances. They are given to you in the hope that a foot ulcer can be successfully treated before an amputation is required. If you are not able to take them as prescribed it is extremely important that you discuss this fully with your doctor so that alternatives or medication to counteract the worst of the side effects can be arranged for you.
The old saying, “An ounce of prevention is worth a pound of cure” has never been more apt when it comes to foot care for diabetics.
Please strive for normal blood sugars and be extra respectful and vigilant when looking after your precious feet.
![]()
Quick Quiz:
1. Regarding your shoes you should do one of these…
a Wear the same pair every day to make the leather softer.
b Buy shoes early in the day when your feet are less smelly.
c Buy shoes late in the day when your feet are more swollen.
d Buy shoes from the internet or from a catalogue to save walking around shops.
2. Nerve damage causes one of these…
a The feet become more sensitive to pain.
b Bacteria and fungus grow between the toes.
c The feet become abnormally sweaty.
d The feet become less sensitive to pain.
3. You should do three of these things to maintain foot health. What one should you avoid?
a Examine them every day using a mirror if necessary.
b Get corns and callouses regularly paired by a podiatrist.
c Rub animal or vegetable oil into the feet daily to keep skin supple.
d See an experienced doctor or nurse immediately if you get a foot injury or infection.
Have you got it?
1. C is true. Dr Bernstein gives comprehensive advice in his book Diabetes Solution about foot care that you may not hear from your diabetic clinic. Neuropathy can develop within five years for type ones and is often present at diagnosis for type twos as they may have been unaware of having the condition for years.
2. D is correct. It is a sad thing but despite the fact that neuropathy pain can become so intense that it needs opiate and anti-epileptic medications to control it, high blood sugars cause the nerves to be less sensitive to touch and external trauma that would cause pain in a non diabetic person’s foot. Bits of gravel, a seam from a sock and simply over tight shoes can cause friction damage that may go unnoticed unless you make the effort to troubleshoot every day.
3. ACD are the right things to do. Removing or paring callouses can increase your risk of infection and therefore amputation. The callous is a sign of too much pressure on that part of the foot. It is much better to PREVENT the possibility of amputation by leaving the callous alone and taking steps to change your footwear or insoles so that it gradually goes itself.
Reference Info:
Most of the information in this section has been obtained from Dr. Bernstein’s Diabetes Solution: The Complete Guide to Achieving Normal Blood Sugars

Overview
The Joslin Diabetes Centre have a check list so you can see what sort of things you need to know to look after yourself with diabetes. This list covers type one and type two diabetes. For each heading I will list what we have already covered on this course and what we will be covering in more depth in the Type One Section *
There is a considerable overlap between both types of diabetes. To start with most people with insulin dependent diabetes diagnosed in childhood or young adulthood are not overweight or insulin resistant. As time goes on this may change so Type Ones would benefit from reading the earlier sections to see if any of it applies to them. The majority of the carb counting methods have also already been covered in the Metabolic and Type 2 section.
For type twos who start off on diet or oral medications they may find that after a while this is no longer sufficient to maintain normal blood sugars. You may benefit by reading on to find out how to deal with insulin now or in the future.
If you don’t feel really confident about any of the things I have listed please take advantage of some of the books and internet resources in the help sections. It is important that you know what to do ahead of any emergency developing so please contact your diabetes support team for further personal training.
MEAL PLANNING
Your own meal plan
know how carbs, proteins* and fats affect the body
special foods and occasions
dining out
portion control
label reading
how to fit in treats*
alcohol*
SELF MONITORING OF BLOOD SUGAR
blood glucose goals
how to use the meter
monitoring schedule*
storing supplies*
interpreting blood glucose values and making decisions in diabetes treatment plan*
USE OF INSULIN AND DIABETES MEDICATIONS
Action and side effects of medication*
timing and schedule*
insulin injection techniques*
storage, refrigeration and disposal of supplies*
what to do if you miss a dose*
EXERCISE
What type, how long, how hard, how often and when.*
snacking adjustments*
preventing high and low blood sugars*
KNOWLEDGE OF HIGH AND LOW BLOOD GLUCOSE
Factors that cause high and low blood glucose*
symptoms*
how to treat*
when to call a healthcare provider*
how to prevent*
FOOT CARE
daily foot care*
emergency treatment for cuts, sores and abrasions.
how to do a proper foot exam*
proper footwear
URINE TESTING FOR KETONES
When and how to check for ketones*
What ketones mean*
When to call a doctor*
YOUR HEALTH TEAM WILL DO THESE ANNUAL CHECKS AND TESTS
A1C ( 2-4 times a year)*
kidney function*
cholesterol, ldl, hdl, triglycerides*
foot exam*
eye exam*
blood pressure*
general health check eg thyroid, tests for coeliac disease and anything relevant to you*
YOU NEED TO BE VERY CONFIDENT ABOUT…
Your own meal plan
The medication you are taking
Your glucose monitoring system*
The treatment of high and low blood sugars*
How to manage your sick days*
Your risk factors for developing other health problems
Your foot care
![]()
Quick Quiz:
1. A test type twos should have done every six months is…
a Liver function and creatine kinase.
b Hbaic.
c Fasting lipids.
d Sex hormone binding globulin.
Have you got it?
1. You must have your hbaic checked every 3-6 months. If statins are being taken, fasting blood lipids, liver and creatine kinase levels may be taken episodically.

Nice blog
LikeLiked by 1 person
Thank you!
LikeLiked by 1 person
My pleasure, followed you 💕
LikeLike