Adapted from Journal of Forensic and Legal Medicine Feb 2023 Insulin murder and the case of Colin Norris by Alan Wayne Jones University of Linkoping, Sweden.
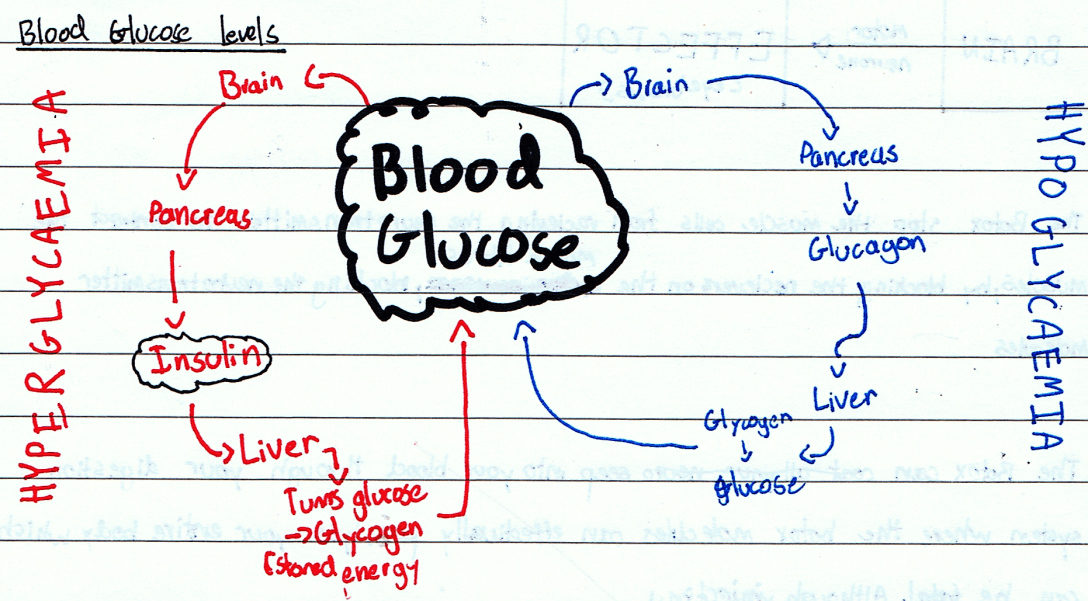
Although insulin is an essential medicine and a life saving drug, it has been used in many poisonings. These can be accidental, suicidal or to deliberately cause harm. An insulin overdose causes severe low blood sugars, and if untreated can lead to coma, irreversible brain damage and death.
Normally, in non- diabetic individuals, the beta cells in the pancreas secrete the same amounts of insulin and C peptide into the portal venous system. In the liver, the insulin is broken down faster than the C peptide, so normally there is more C peptide in the general circulation than insulin. When there is more insulin in the system than C peptide, that is a very strong indicator that insulin from a non- pancreatic source has been administered.
Sophisticated biochemical measuring systems can identify insulin analogues. This provided part of the evidence that convicted Colin Norris, a nurse, of injecting insulin into five of his patients, four of whom died as a result.
Clinical symptoms of low blood sugars occur when the blood sugars drop below 2.5 (UK) or 45 (USA), although the exact threshold can vary between individuals. If this is prolonged for up to 6 hours or more then the brain damage can be irreversible and death can occur. The hormonal response to correct low blood sugars also prolongs the QT interval in the heart electrical pacing mechanism leading to an increase in cardiac arrhythmias and sudden death.
Proof of insulin poisoning requires positive identification of the causative agent in plasma or serum samples taken from the victim before the low blood sugar is corrected.
The first proven case of murder by insulin occurred in the mid 1950s and forensic evidence was obtained from analysing tissue samples from around injection marks on the victim’s buttocks.
During an investigation into suspicious deaths caused by insulin, the entire case scenario and totality of the evidence must be carefully considered. Tissue samples around any injection marks need to be kept for later analysis of insulin and C peptide levels.
In a Leeds hospital, in September 2002, a Mrs Hall was recovering from a hip joint operation and seemed to be making good progress. In the early hours she was found unresponsive. A bedside test showed that her blood sugar was only 1.5. Although intravenous dextrose was given, she never regained consciousness and later died. She did not have diabetes. Assays showed that the insulin level was far higher than the C peptide level indicating that pharmaceutical insulin had been injected. It was believed that she may have been mistakenly injected with insulin which was kept for patients in an unlocked fridge.
Nurse Colin Norris became the prime suspect. As part of the investigation a retrospective review of other unexpected deaths and incidents which could have been due to insulin administration were found. Four incidents had occurred in the previous year when Colin Norris was on duty. Three earlier deaths had been attributed to natural causes at the time and there was no toxicological evidence that any of them had been injected with insulin. Colin Norris maintained his innocence throughout the investigation.
In October 2005 Colin Norris was charged with murdering four patients and attempting to murder a fifth by the injection of insulin. The trial started at Newcastle Crown Court in October 2007. In March 2008 he was found guilty and was sentenced to life imprisonment. He was described by the judge as a “thoroughly evil and dangerous man…arrogant and manipulative….with a real dislike of elderly patients. There cannot be any suggestion that you were motivated to hasten their ends to spare them suffering”.
After the first appeal against Norris’s conviction failed in 2009, clinical evidence emerged that spontaneous attacks of hypoglycaemia in elderly and frail patients are not as rare as the jury had been led to believe. Indeed, a literature review showed that 2-10% of elderly frail patients, who can be malnourished, with co-morbidities such as sepsis, liver disease, or kidney failure are vulnerable to attacks of hypoglycaemia.
Other weaknesses in the case were:
The insulin vials on the ward were not subject to any inventory.
No insulin or needles were found near Mrs Hall.
The fingertip blood sample showing low blood sugar was not verified with a venous blood sample.
The very high insulin level was found on an NHS assay machine, not a more accurate forensic one. Rigour in following chain of custody procedures were not done. A confirmatory sample had also not been done.
The low blood sugar had been corrected before the low C peptide versus high insulin was found.
Spontaneous hypos can indeed occur in the elderly and frail.
Another hypoglycaemia related death had occurred at the hospital but it had not been mentioned as Norris had not been on duty. Thus the police were suspected of cherry picking cases to incriminate Norris.
Toxicological evidence of hypoglycaemia was only found for Mrs Hall. Death certificates for the other suspected hypoglycaemia deaths had been attributed to old age and other natural causes.
The cause of death of Mrs Hall was brain damage due to insulin induced hypoglycaemia but it was not known if the pathologist had looked for any insulin secreting tumours.
One of the senior police officers had been involved in the Dr Harold Shipman case two years previously and he may have been primed to find another serial killer in the health profession.
The Criminal Case Review Committee, which is the official authority in the UK charged with looking into miscarriages of justice, have examined the evidence and recommended that the court of appeal have a fresh look at the case.
My comment: It will be interesting to find out what happens and what their reasoning regarding this case will be. Meanwhile, look after yourself, look after your diabetes, keep up a healthy lifestyle and keep out of hospital!