A Complete Guide to the Keto Diet
by Chris Kresser
Published on April 2, 2019
Ketogenic diets are currently all the rage. Seemingly every health personality has an opinion on the ketogenic diet, commonly referred to as “keto.” Some tout it as a cure-all for everything from diabetes to cancer, while others express skepticism or disagree with some aspects of the diet.
The keto diet could help alleviate conditions like obesity and type 2 diabetes and even impact the progression of some types of cancer, but it isn’t for everyone.
It’s understandable that you may be wondering how to sort out the facts and interpret the latest research. Who is a good candidate for keto, and who should avoid it? How does someone successfully adhere to a ketogenic diet? In this article, I’ll answer these important questions and others so you can make an educated decision about whether keto is right for you.
What is the keto diet?
Nine conditions that respond well to keto
Who should avoid the diet
The keto time frame
Three steps to starting keto
13 tips and tricks
What to expect on keto
What Is the Keto Diet?
The ketogenic diet is a high-fat, moderate-protein, low-carb food plan. The typical macronutrient ratios are 60 to 75 percent of calories from fat, 15 to 30 percent of calories from protein, and 5 to 10 percent of calories from carbohydrates.
By strictly limiting dietary carbohydrates, the ketogenic diet encourages the body to switch from using glucose as a primary fuel source to burning body fat and using ketones for fuel. This metabolic switch has a variety of beneficial effects on the body, ranging from fat loss to improved brain function.
The keto diet could potentially address a number of health conditions, such as obesity, type 2 diabetes, and even cancer. Check out this article for more information on who should try keto—and who shouldn’t—and get tips to help you. #lowcarb #nutrition #chriskresser
A ketogenic diet differs dramatically from the carbohydrate-heavy Standard American Diet. When you eat a carbohydrate-rich meal, the ingested carbs are broken down into glucose. Glucose is then shuttled into cells by insulin, where it is used for energy production. The constant consumption of a high-carbohydrate diet causes the body to rely on glucose (sugar) for fuel, while rarely tapping into fat stores for energy. A ketogenic diet does just the opposite. It forces the body to turn to fats for fuel. A keto diet encourages the production of ketones, small water-soluble compounds, and the “burning” of fatty acids in adipose tissue (fat cells) for energy. Ketones are unique in that they are rapidly taken up by tissues and broken down to yield ATP, the primary energy currency of the human body. The process by which the body switches to using ketones for energy is referred to as “nutritional ketosis,” while the process of tapping into your body’s fat stores is termed “fat adaptation.”
Choosing the right diet can be a difficult process of trial and error. Health coaches support people in finding the best diet for their bodies, lifestyles, families—wherever they need encouragement in discovering the right path, etc. As a coach, you learn to ask the questions that help people figure out whether a diet is the right fit for them. This not only helps them make a good choice but minimizes the time they spend with diets that don’t work well for them.
Health coaches can also help people navigate their chosen diets, like the ketogenic diet. As an example, some people may need a little extra push getting their bodies to transition to using ketones. If you are finding it difficult to get into ketosis, a health coach can help you navigate that process.
How do health coaches do this? In our ADAPT Health Coach Training Program, you learn about a variety of diets—including the ketogenic diet—how they work, who they work well for, and how to support people in making diet transitions. Visit our health coach training program page to find out more.
The ADAPT Health Coach Training Program is an Approved Health and Wellness Coach Training & Education Program by the National Board for Health and Wellness Coaching (NBHWC).
Nine Conditions That Are Ideal for Keto
The ketogenic diet offers many health benefits, but it isn’t right for everyone. Read on to learn who stands to benefit the most from keto and which conditions tend to respond the best to the diet.
1. Obesity
Disturbing statistics indicate that weight problems have reached epidemic proportions in the United States, with nearly 72 percent of American adults 20 and over categorized as overweight or obese. (1) The mandate that overweight and obese individuals should merely “eat less and exercise more” is failing miserably; it does little to correct the underlying metabolic disturbances driving obesity, trapping people in a vicious cycle of weight loss and regain. However, all hope is not lost! The ketogenic diet is emerging as a powerful, sustainable tool for weight loss in overweight and obese individuals.
A growing body of research indicates that ketogenic diets are more effective than low-fat diets for sustaining long-term weight loss in obese adults. (2, 3) Furthermore, the weight loss observed on a ketogenic diet is primarily visceral fat, the hard-to-lose fat located deep in the abdominal cavity; lean body mass, on the other hand, is preserved. (4)
A ketogenic diet may also benefit obese children. A study that placed obese children on a ketogenic diet for six months observed significant decreases in body fat, waist circumference, fasting insulin levels, and HOMA-IR, a marker used to detect insulin resistance. (5)
The ketogenic diet facilitates fat loss by increasing the efficiency of fat oxidation (the process by which fat is “burned” for energy), suppressing hunger hormones, and providing the body with plenty of satiating dietary fat and protein, thus decreasing total energy intake. (6)
For those who do not wish to stay on the ketogenic diet long term, a cyclic ketogenic diet alternated with a nutrient-dense, whole foods diet can also lead to successful long-term weight loss. (7) I’ll cover the cyclic ketogenic diet in more depth shortly.
2. Metabolic Syndrome
Over one-third of Americans have metabolic syndrome, a constellation of complications including increased blood pressure, elevated blood sugar, excess abdominal fat, and abnormal triglyceride and cholesterol levels that significantly increase one’s risk of heart disease, diabetes, and stroke. (8) The conventional treatment of metabolic syndrome typically involves cholesterol-, blood sugar-, and blood pressure-lowering medications, along with vague advice to “eat better.” Given that heart disease is still the number one cause of death in the United States, that diabetes is considered to be at epidemic proportions, and that strokes disable or kill someone every 40 seconds on average, this treatment paradigm leaves much to be desired. (9)
Fortunately, patients have an alternative—a ketogenic diet. Research indicates that a ketogenic diet improves multiple aspects of metabolic syndrome, inducing significant reductions in body fat percentage, BMI, hemoglobin A1c levels, blood lipids, and blood pressure. (10, 11, 12) The ketogenic diet produces these beneficial effects by reversing the pathological processes underlying metabolic syndrome, including insulin resistance and chronic inflammation.
3. Type 2 Diabetes
Ketogenic diets represent a far more effective strategy for managing type 2 diabetes than the American Diabetes Association’s high-carb, low-fat dietary guidelines. Unlike the ADA’s guidelines, a ketogenic diet significantly reduces blood sugar, hemoglobin A1c levels, waist circumference, and triglycerides in diabetic individuals. (13) Most importantly, research indicates that the diet is sustainable for diabetic patients and that the beneficial changes can be maintained over the long term. (14)
4. Polycystic Ovary Syndrome (PCOS)
Between 5 and 10 percent of women in the United States have polycystic ovary syndrome (PCOS), a disorder characterized by insulin resistance, menstrual irregularities, hyperandrogenism, overweight, and obesity. (15) A ketogenic diet improves fertility in women with PCOS by improving insulin resistance, promoting weight loss, and inducing ovulation. (16)
5. Neurodegenerative Diseases
A great deal of exciting research is emerging regarding the application of a ketogenic diet in the treatment of neurodegenerative diseases, including Alzheimer’s and Parkinson’s disease. (17) Neurodegenerative diseases are characterized by brain insulin resistance, a condition that starves neurons of the glucose they normally need to function correctly. Scientists have found that ketones are an excellent alternative fuel for the insulin-resistant brain. In addition, ketones reduce brain oxidative stress and mitochondrial dysfunction, two significant factors in the neurodegenerative disease process.
Animal research indicates that a ketogenic diet reduces levels of brain amyloid-beta, a misfolded protein that contributes to Alzheimer’s disease, while also restoring mitochondrial function and improving learning and memory. (18, 19, 20) Although fewer studies on a ketogenic diet have been done in humans with Alzheimer’s disease, a recent trial found a ketogenic diet to be both safe and effective for mild Alzheimer’s disease. (21)
Preclinical research suggests that a ketogenic diet may also benefit those with Parkinson’s disease. In animal models of Parkinson’s, a ketogenic diet improves motor function, and in humans with Parkinson’s, it improves nonmotor symptoms such as daytime sleepiness and cognitive disorders. (22, 23) While more research is needed, a ketogenic diet may be a powerful intervention well worth a try for both Alzheimer’s and Parkinson’s patients.
6. Traumatic Brain Injury and Epilepsy
Traumatic brain injury (TBI) is an injury caused by a blow, bump, or jolt to the head that significantly impairs brain function. TBI is common in military personnel, car accident survivors, and athletes involved in contact or high-risk sports. If left untreated, TBI can cause severe impairments in thinking, memory, and emotional regulation. Interestingly, a ketogenic diet may be an effective strategy for reducing the harmful effects of TBI.
A ketogenic diet promotes healing of the brain following TBI by increasing the activity of genes genes involved in energy metabolism, stimulating the generation of new mitochondria, and inhibiting the production of damaging reactive oxygen species in the brain. (24) In animal models of TBI, a ketogenic diet reduces cerebral edema and neuronal cell death while improving behavioral outcomes. (25, 26) While individual success stories of people using a ketogenic diet for TBI are easy to find on the internet, formal clinical trials are still needed.
Compared to TBI, the amount of scientific literature documenting the beneficial effects of a ketogenic diet for epilepsy is vast. The ketogenic diet was first introduced as a therapy in the 1920s, when doctors learned it could successfully treat seizures in children with refractory epilepsy. (27) Interest in the ketogenic diet waned when antiepileptic drugs were introduced in the 1960s and ’70s; however, the ketogenic diet has experienced a recent resurgence in popularity in the epilepsy community, particularly among those suffering from drug-resistant epilepsy.
The ketogenic diet exerts antiepileptic effects by improving energy metabolism in the brain and reducing brain oxidative stress. Fascinating new research suggests that the antiseizure effects of the ketogenic diet are also mediated by modulation of the gut microbiota. (28) Consumption of a ketogenic diet increases the levels of bacteria that produce GABA, the brain’s primary inhibitory neurotransmitter; this shifts neurotransmission towards inhibition rather than excitation, thus preventing neuronal hyperexcitability and seizure onset.
7. Digestive Disorders
A high carbohydrate intake can exacerbate irritable bowel syndrome (IBS) and gastroesophageal reflux disease (GERD) by feeding opportunistic and pathogenic bacteria in the gut. (29) These microbes ferment dietary carbohydrates, producing gases that increase intraabdominal pressure, a driving force behind acid reflux and GERD. The gas manufactured by these bacteria also contributes to bloating, abdominal pain, and diarrhea in IBS.
How can a ketogenic diet help with IBS and GERD? By significantly reducing dietary carbohydrate load, a ketogenic diet provides less fermentable substrate for gut bacteria, reducing the amount of gas produced in the small intestine. Several small studies indicate that a ketogenic diet improves abdominal pain, stool frequency, and reflux in patients with IBS-D and GERD, respectively. (30, 31) However, it is important to note that the long-term effects of a low-fermentable-carbohydrate diets, including the ketogenic diet, on gut bacteria remain to be seen. Our beneficial gut bacteria also require fermentable carbohydrates to survive, so it’s possible that the ketogenic diet could reduce their numbers. This is why I highly recommend following a cyclic ketogenic diet rather than a long-term, strict ketogenic diet. I’ll provide more information on that topic shortly.
8. Skin Conditions
A ketogenic diet may seem like an unlikely approach for treating skin issues. However, keto addresses several of the physiological mechanisms underlying dermatological issues, particularly acne and psoriasis, and can therefore help people correct the root cause of their skin conditions.
Insulin is a crucial driver of acne due to its effects on hormones, sebum production, and inflammation. By reducing insulin, the ketogenic diet may correct hormone imbalances, excessive sebum production, and inflammation, thereby alleviating acne. (32)
High blood sugar promotes psoriasis by increasing levels of a protein that causes inflammation. A ketogenic diet corrects hyperglycemia and may lower the level of this protein, resulting in the amelioration of psoriasis. (33)
9. Some Forms of Cancer
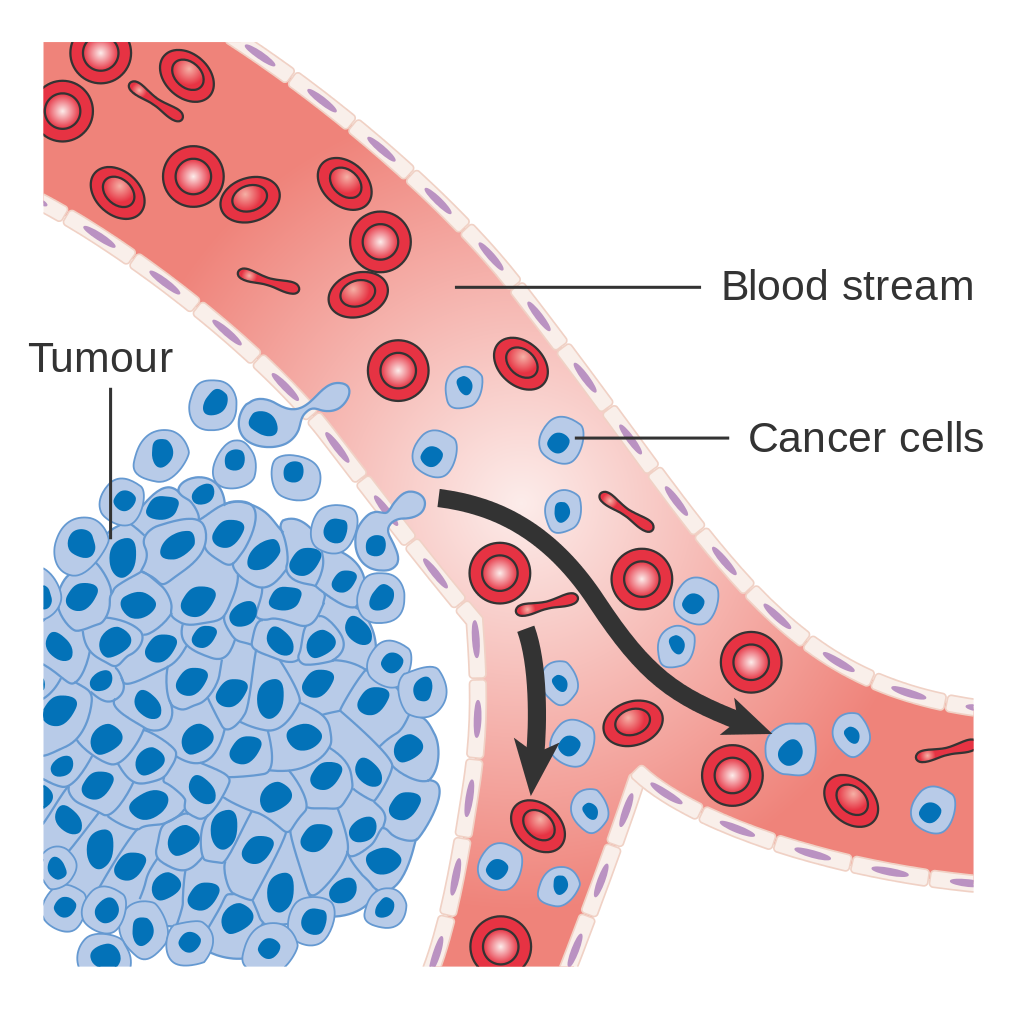
Some of the most exciting research on the ketogenic diet pertains to its applications in the treatment of cancer. A rapidly growing collection of animal studies indicates that the ketogenic diet has anticancer effects in malignant glioma, neuroblastoma, prostate cancer, and colon cancer. (34) In humans, a ketogenic diet has been found to work synergistically with antineoplastic agents in the treatment of malignant glioma, a common primary brain tumor that is notoriously difficult to treat. (35) Several small studies indicate that the ketogenic diet improves body weight and blood profiles while reducing a marker for tumor progression, TKTL1, in patients with breast, prostate, colon, melanoma, and lung cancers. (36, 37)
The ketogenic diet exerts anticancer effects by inducing a metabolic shift in malignant tissues that promotes apoptosis (self-programmed death) of cancer cells, inhibiting angiogenesis (the growth of new tumor-supporting blood vessels), reducing oxidative stress and inflammation, suppressing mTOR (a protein in humans involved in the regulation of cell growth and regeneration), and increasing the sensitivity of certain cancer cell types to chemotherapy. (38)
Since a ketogenic diet can induce weight loss, clinicians should take care to ensure that adequate calories are consumed to inhibit undesirable weight loss in cancer patients.
It is crucial to recognize that not all forms of cancer will respond to a ketogenic diet.
Research suggests that cancer cells with low levels of particular enzymes (the ketolytic enzymes 3-hydroxybutyrate dehydrogenase and succinyl CoA 3-oxoacid CoA transferase) are more susceptible to the anticancer effects of a ketogenic diet. Screening a patient’s cancer cells for these enzymes may represent a valuable strategy for determining whether a ketogenic diet may be of use. (39)
Who Should Avoid a Ketogenic Diet?
The ketogenic diet is not appropriate for everyone. If you fit any of the descriptions listed below, then a ketogenic diet may have a negative impact on your health.
You Have a Genetic Condition That Affects Fatty Acid Metabolism
Since fats are consumed in large quantities on a ketogenic diet, any genetic condition that impairs fatty acid metabolism precludes the use of this diet. If you have primary carnitine deficiency, pyruvate carboxylase deficiency, or any of the other genetic conditions listed here, a ketogenic diet is absolutely contraindicated.
You’re Pregnant or Breastfeeding
While a growing fetus can utilize ketones to an extent, it still requires a steady glucose supply to support normal growth, including crucial brain development. Reduced glucose availability caused by a maternal ketogenic diet may have long-term adverse effects on infant health, including abnormal growth patterns and alterations in brain structure. (40) If you are pregnant and struggling with blood sugar issues, a low-carbohydrate diet that includes moderate amounts of nutrient-dense carbohydrates, such as fruit and starchy tubers, is a safer choice than a ketogenic diet.
You Have Gallbladder Disease or No Gallbladder
The body needs bile to break down and digest dietary fat, and the gallbladder is responsible for storing bile before its release into the small intestine. Removal of the gallbladder and gallbladder disease cause fat malabsorption and may make it difficult to follow a ketogenic diet. If you have had your gallbladder removed or have existing gallbladder disease, consult with your doctor before trying a ketogenic diet.
You’re Suffering from Kidney Disease or Kidney Stones
While preliminary research suggests that a ketogenic diet may benefit chronic kidney disease patients, caution is advised in those with kidney disease or kidney stones. (41) If you have a kidney condition, consult with your doctor before starting a ketogenic diet.
You Have HPA Axis Dysfunction and High Levels of Stress
A ketogenic diet has been observed to raise cortisol, the body’s primary stress hormone. If you struggle with high levels of stress or HPA axis dysfunction, a ketogenic diet may push your stress-response system into overdrive and cause burnout. A diet that includes a moderate intake of carbohydrates is typically a better fit for those with high-stress lifestyles or HPA axis dysfunction.
You’re a Hyper-Responder to Dietary Cholesterol
While dietary saturated fat and cholesterol do not impact blood cholesterol levels in most people, they may raise total and LDL cholesterol in a subset of the population referred to as “hyper-responders.” If you are a hyper-responder (this is something you’ll need to determine with the help of your doctor), I recommend following a Mediterranean Paleo-style diet, an approach that is lower in fat and higher in Paleo-friendly carbohydrates, rather than a ketogenic diet.
You’re an Athlete
If you participate in exercise that involves explosive movements such as jiujitsu, mixed martial arts, CrossFit, or even some rigorous forms of dance, you may benefit from a moderate carbohydrate intake rather than a ketogenic diet. Explosive movements draw on your muscles’ glycolytic capacity, which is powered by glucose from dietary carbohydrates. Endurance athletes, on the other hand, may thrive on a ketogenic diet because their respective activities can be adequately fueled by fatty acid oxidation and ketones.
How Long to Follow the Ketogenic Diet
The ideal keto diet time frame must take into account both nutritional ketosis and fat adaptation. Ketosis means your body is experiencing an acute lack of glucose and is therefore producing ketone bodies for energy. Fat adaptation, on the other hand, means your body has become adapted to burning fat for fuel.
When you first embark on a ketogenic diet, your goal is to be in nutritional ketosis consistently. Over time, as you train your body to function on fewer carbohydrates, you may enter the fat adaptation phase. While ketosis can be achieved after just a few days of the diet, at least three to four weeks of strict adherence to the diet is required in order to reach the fat adaptation state. This is also the time frame during which you’ll likely begin to notice benefits of the diet.
While some keto proponents advocate following the diet long term, a cyclic ketogenic diet may be a healthier choice.
A cyclic ketogenic diet involves carb-loading one to two days of the week, followed by a standard low-carb ketogenic diet the remaining days of the week. Cyclic keto has many benefits—it allows the body to enter a state of ketosis regularly while also satisfying carb cravings, improving sleep, and promoting a healthier balance of gut bacteria.
The Three-Step Process to Starting Keto
Step 1: Find Your Macronutrient Ratio
The goal of a ketogenic diet is to transition the body’s primary fuel supply from carbohydrate to fat, creating a state of nutritional ketosis and, eventually, fat adaptation. The degree to which dietary carbohydrates need to be reduced to reach nutritional ketosis varies from person to person. Finding the optimal macronutrient ratios for getting your body into ketosis requires some self-experimentation. I recommend playing around with the ranges listed below to find the ones that work best for you.
Possible macronutrient ranges for keto:
60 to 75 percent of calories from fat
15 to 30 percent of calories from protein
5 to 10 percent of calories from carbohydrates
I would like to emphasize that the super-high-fat, low-protein version of keto promoted by some keto advocates is not necessary for most people to obtain the benefits of keto.
Proponents of the super-high-fat, low-protein approach argue that protein kicks the body out of ketosis by supplying amino acids for gluconeogenesis (simply put, turning non-carbs into fuel); however, research indicates that the impact of dietary protein on gluconeogenesis and glucose flux is nearly negligible, making this argument irrelevant.
(42) In my practice, we have found that usual protein intakes (15 to 20 percent of calories) do not have appreciable effects on blood ketone levels. Besides, a super-high-fat, low-protein diet typically has more drawbacks than benefits—it may cause weight gain, muscle loss, fatigue, and chronic hunger. Don’t be afraid of including plenty of protein in your ketogenic diet; protein is a powerful tool that will satiate your appetite while facilitating fat loss and preventing muscle loss.
Step 2: Don’t Count Calories
I don’t recommend counting calories on the keto diet. Tracking your macronutrients, on the other hand, can be helpful. Try using an app for journaling your food intake and obtaining your ratios of macronutrients. I recommend the Carb Manager Keto Diet App.
Step 3: Regularly Test Your Ketones
To determine whether you’re in ketosis and what degree of ketosis you’re in, test your ketones each morning. Blood ketone testing is the most accurate method—I do not recommend breath or urine ketone monitoring. In our practice, we recommend the Precision Xtra Blood Glucose Meter Kit, which can be purchased on Amazon (you can buy test strips for this meter in bulk on eBay for a lower cost). Keto Mojo is another good meter with affordable test strips.
If your ketone value is above 0.5 mmol/L first thing in the morning, you’re in ketosis. However, a range of 0.7 to 2.0 mmol/L is optimal for most people. If your value is above 3.0 mmol/L, you may not be eating enough and/or should consider adding some carbohydrates back to your diet. However, in the long run, your goal should not be a specific number on the ketone meter, but an improvement in your symptoms.
13 Tips and Tricks to Help You Follow a Ketogenic Diet
Following a ketogenic diet can take some work and planning. Here are some tips and tricks to help you get into ketosis faster.
1. Eat Enough Calories and Protein
Failing to consume enough calories on a keto diet can cause fatigue and insomnia, while an insufficient protein intake promotes weight gain and muscle loss. When you first begin a keto diet, it can be helpful to track your food intake with an app such as Carb Manager Keto Diet App; this will allow you to visualize your macronutrient intake and ensure that you don’t undereat calories or protein. As I mentioned earlier, a low-protein intake is not required to obtain the benefits of keto. A sufficient protein intake (15 to 30 percent of total calories) suppresses hunger and, in most people, does not affect blood ketone levels. (43)
2. Add Supplemental Fat
Fat is the primary source of fuel on a ketogenic diet, and supplementing with specific types of fat, particularly coconut oil and medium-chain triglyceride (MCT) oil, can help you get into ketosis faster. MCT oil is unique in that it increases ketone levels in a linear, dose-dependent manner and allows for the induction of ketosis with lower amounts of total fat in the diet. (44)
If you are a hyper-responder to dietary fat and cholesterol, you may need to restrict your intake of saturated fats on keto. Instead, focus on fats such as olive oil, avocados, fatty fish, nuts, and seeds.
3. Supplement
L-leucine is a ketogenic amino acid, meaning it can be used to make ketones. Supplementing with L-leucine may help you get your body into ketosis faster.
Exogenous ketones are ketones that are ingested as a nutritional supplement. They elevate blood ketone levels but may inhibit the body’s own process of ketogenesis. (45) I consider exogenous ketones an advanced strategy for those who have already nailed down the basics of keto.
4. Drink Apple Cider Vinegar
Consuming apple cider vinegar before meals not only assists digestion but may also promote ketone production due to its content of acetic acid, a naturally occurring ketogenic compound. Try adding a tablespoon or two to water and drinking before you eat your meal.
5. Increase Your Salt Intake
The body excretes more salt on a keto diet than on a standard diet due to reductions in insulin, which normally promotes a certain degree of water retention. Once you’re in ketosis, add an extra three to five grams of Himalayan, sea, or Redmond Real salt to your diet every day. (Five grams is about one teaspoon, but that may vary depending on the type of salt and the size of the grain.)
6. Eat More Magnesium and Potassium
In addition to sodium, levels of magnesium and potassium can also drop on a ketogenic diet due to its dehydrating effect on the body. Make sure to eat plenty of magnesium- and potassium-rich foods. Some of the best keto-friendly sources of magnesium are dark leafy greens, nuts and seeds, and cacao. Keto-friendly potassium sources include spinach, kale, avocados, and mushrooms.
7. Avoid Artificial Sweeteners
Artificial sweeteners such as saccharin (Sweet’N Low), aspartame (NutraSweet, Equal), and sucralose (Splenda) are quite popular among low-carb dieters. However, concerning new research indicates that artificial sweeteners have adverse metabolic effects and may work against your keto efforts by disrupting your gut microbiota and inducing insulin resistance and weight gain. (46, 47) If you want to use a non-caloric sweetener, I recommend either stevia or monk fruit sweetener.
8. Stock Up on Keto-Friendly Snacks
Keep keto-friendly snacks on hand so that when hunger strikes, you have healthy food at the ready; this strategy will help prevent you from falling off the keto wagon and reverting to high-carb snack foods. Nuts and seeds, coconut butter, grass-fed beef jerky, and hard-boiled eggs make for easy, portable keto snacks.
9. Try Intermittent Fasting
Intermittent fasting, an eating style in which you eat within a specific period each day and fast the rest of the time, is a great way to reduce the amount of time your body needs to enter nutritional ketosis. (48) Intermittent fasting accelerates the time to ketosis by keeping insulin levels low and raising ketone levels. If you’re new to intermittent fasting, start by limiting your eating to an eight- to 10-hour window each day and fasting for the remaining 14 to 16 hours of the day (and night).
10. Decrease Your Stress
Stress is an underappreciated but significant impediment to achieving success on a ketogenic diet. High stress elevates cortisol, which stimulates the generation of glucose (gluconeogenesis) in the liver. Gluconeogenesis raises blood glucose and reduces ketone levels; together, these effects make it difficult to enter ketosis.
Try these strategies for reducing your stress:
Set aside time for rest, ideally away from your smartphone and computer
Cut down on commitments
Get plenty of sleep
Start a mindfulness practice such as meditation
Spend time in nature
Spend quality time with friends and family
11. Prioritize Sleep
Inadequate sleep will rapidly derail your keto efforts by increasing your blood sugar and levels of stress hormones. Getting eight to nine hours of high-quality sleep per night should be a priority. Maintain a regular bedtime schedule and practice sleep hygiene strategies such as keeping your bedroom completely dark at night, lowering the ambient temperature to around 67 degrees Fahrenheit, and avoiding blue light exposure a couple of hours before bed with blue light-blocking glasses.
12. Exercise
Frequent exercise depletes glycogen stores, causing your body to turn to fat for energy; this means that regular exercise can help you get into ketosis faster. Some people experience a reduced capacity for exercise upon starting keto; in this case, engaging in longer durations of low-intensity activity, such as walking, cycling, or swimming, can help you get into ketosis without causing undue fatigue.
13. Drink Plenty of Water
Within the first few days of starting a ketogenic diet, you may experience a significant loss of water weight. This occurs primarily because glycogen stores in muscle are gradually being reduced, and glycogen causes retention of water. To ensure that you don’t become dehydrated on keto, drink half your weight in ounces of filtered water every day.
What to Expect When You’re on the Keto Diet
As your body gets used to keto, you may experience some uncomfortable side effects. Here’s what to expect.
The “Keto Flu”
The first few days of keto can be difficult as your body adjusts to a low carbohydrate intake; you may experience symptoms such as brain fog, headache, insomnia, irritability, and digestive issues. These symptoms are commonly referred to as the “keto flu” and are caused by the glycogen loss, low insulin levels, and dehydration that frequently occur when you suddenly cut back on carbs. Know that these symptoms will pass, especially if you make sure to drink plenty of water, replenish your electrolyte levels, and eat sufficient protein and calories. At the most, it may take a couple weeks for the keto flu to subside, but for most people, this uncomfortable period passes within a few days.
Constipation
Constipation is a common complaint for keto dieters. There are several reasons why you may experience constipation:
You’re not eating enough fiber. It’s easy to eat lots of meat, cheese, and oils on a ketogenic diet at the expense of optimal fiber intake. Be sure to eat plenty of colorful non-starchy vegetables (broccoli, cauliflower, kale, bell peppers, mushrooms) because the fiber in these foods will keep things moving through your digestive tract.
You may need more water. As I mentioned earlier, people typically experience body water loss when starting a ketogenic diet. Your digestive tract needs water to keep fecal matter soft and moving through your intestines; if you are dehydrated, constipation is likely.
Try resistant starch. Resistant starch passes through the small intestine intact and therefore doesn’t count as a dietary carbohydrate. Instead, it travels to your large intestine, where it’s used to feed beneficial gut bacteria. Try adding a teaspoon of resistant starch, such as raw potato starch or green banana flour, to your keto smoothie each day to keep your gut happy.
Take a probiotic and eat fermented foods. The beneficial bacteria in probiotics and fermented foods help prevent sluggish digestion and promote healthy bowel function.
Reduced Thyroid Function
Research has found that a ketogenic diet decreases levels of T3, the body’s active thyroid hormone. (49) Unfortunately, this means a ketogenic diet may not be optimal for those with pre-existing hypothyroidism. If you have hypothyroidism and want to proceed with a ketogenic diet, consult with your doctor first because you may need thyroid support.
Elevated Cortisol
Research has indicated that a ketogenic diet raises the stress hormone cortisol to increase energy levels in the face of reduced carbohydrate availability. However, it is still up for debate whether this increase in cortisol is harmful or innocuous. Nonetheless, I recommend taking extra care to manage your stress while on a ketogenic diet. Getting plenty of sleep, exercising, and engaging in a regular stress-reduction practice can help you keep your baseline stress levels low and reduce the potential for chronically elevated cortisol.