This question is a lot trickier health wise than you think. There has been new research on a variety of beverages that show various harms and benefits.
Coffee
A study from Cambridge suggests that coffee in itself is not a dangerous drink but that thermal damage to the oesophagus is the problem that can result in a higher risk of oesophageal cancer.
In the UK we drink 98 million cups of coffee each day. There are 67 million adults and children in the UK at present to put this into context.
Tea
Green tea is known to confer some health benefits and a recent prospective study has shown benefit for black tea drinkers too. Half a million UK participants in the Biobank cohort were assessed. There is a moderately reduced all-cause mortality reduction in those who have two or more black teas a day. There also was a reduction in mortality from cardiovascular disease, ischaemic heart disease and stroke. There was no effect on cancer mortality or respiratory disease. Surprisingly given the coffee study, there seemed to be no effect from the temperature of the drink or the addition of milk or sugar.
It is thought that substances in the tea improve endothelial function and this is the cause of the effect.
Pre-meal whey protein drink
A small whey protein pre-meal drink taken 10 minutes before meals, significantly reduces mean blood glucose concentration and for diabetic subjects, the amount of time they spend in normal blood sugar ranges.
A placebo RCT was done on 18 people who had type two diabetes who had never been treated with insulin. They were given a 100ml drink containing 15.8g of protein to be taken ten minutes before breakfast, lunch and dinner.
The protein drinkers significantly reduced the prevalence of hyperglycaemia over the day, increased the amount of time in the normal blood sugar range by around 2 hours extra a day, and reduced the 24 hour glucose concentrations. There was no effect on night time blood sugar levels. The acceptability levels of this were high at 98%.
The researchers at Newcastle University say that the protein seems to slow down the speed of gastric emptying and stimulating hormones that reduce the spike in blood sugars.
Alcohol containing drinks
Alcohol is a major preventable risk factor for cancer. About 4-5% of cancers are alcohol related. A new study suggests that reducing alcohol intake reduces the risk of getting an alcohol related cancer in a Korean study.
Those who drink three or more alcohol containing drinks a day are at particular risk of cancer. The heavier drinkers at the outset have the most to gain by cutting down. Some cancers are much more likely from alcohol than others. More than 45 % of mouth and throat cancers are drink related, 25% of laryngeal cancers, 12% of female breast cancers, 11% of colorectal cancers, 10.5% of liver cancers and 7.7% of oesophageal cancers.
Health screenings in Korea were done in 2009 and 2011. The average age was 53 years and they were followed up for just over six years. Over that time, new cancers were seen in 7.7 per thousand of the 4.5 million people screened.
Those who increased their alcohol consumption had a higher increase in cancers. Those who lowered their alcohol intake lowered their risk. The risks were dose related.
Fruit juice, fizzy pop and diet soda
Drinks sweetened with sugar but not natural juices or artificially sweetened drinks were related to a higher risk of inflammatory bowel disease in people who drank more than one a day, in a study of more than 120,000 people.
66% of the people did not drink any sugar sweetened beverages a day but those who consumed more than one such drink a day had a higher BMI and consumed higher amounts of total energy and sugar.
The participants were followed up over ten years. There was a significant increased risk for Crohn’s disease but not for Ulcerative Colitis in the sugary drink consumers. Diet drinks or natural fruit or vegetable drinks had no effect.
All the subjects were over the age of 40 so the effect on the younger population was not studied. Dr Hasan Zaki said that this would be of interest to study because children consume a lot of sugary drinks and the incidence of inflammatory bowel disease in children increased by a third between 2007 and 2016.
My comment: I was pleased to see the beneficial effects of black tea because I drink about 4 pints of it a day. I do like a glass or two of wine with my dinner, but maybe I should cut this down and have a tomato juice or just plain water instead? The pre-meal protein drink looks interesting. I would expect that it would reduce the amount of food consumed at each meal as it should blunt the person’s appetite. I wonder what the longer term effects on weight would be?
 You find me, un-sensored and sad… Yes, I’ve completed two weeks on the FreeStyle Libre sensor and reader system, and now I’m back to finger pricks, at least temporarily.
You find me, un-sensored and sad… Yes, I’ve completed two weeks on the FreeStyle Libre sensor and reader system, and now I’m back to finger pricks, at least temporarily.
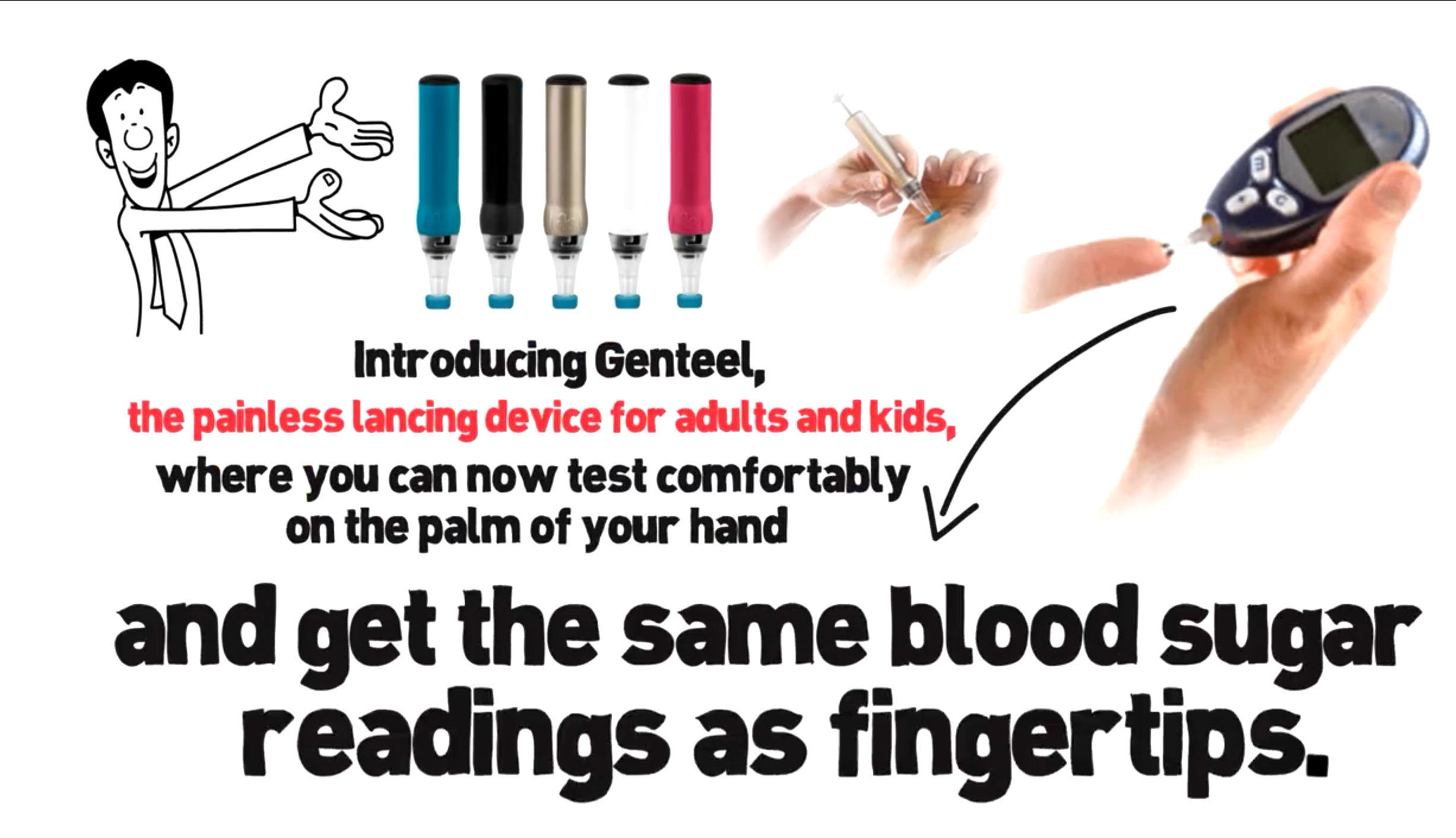 The USA company Genteel have developed a new lancet device that is reported to be painless and can be used successfully for blood sampling in a variety of sites. It is only available in the USA but can be shipped from there. It does cost $129 plus lancets and postage so it does not come cheap. The manufacturers explained how the new device has a role in diabetes management….
The USA company Genteel have developed a new lancet device that is reported to be painless and can be used successfully for blood sampling in a variety of sites. It is only available in the USA but can be shipped from there. It does cost $129 plus lancets and postage so it does not come cheap. The manufacturers explained how the new device has a role in diabetes management….