In part 1, I have discussed the use of ‘healthy’ and ‘all natural’ statements on the food labels. Now I will talk about the labels that claim low or no fat or sugar.
3. No Sugar Added.
This sounds rather confusing, because it prompts you to think that the product contains no sugar at all. If you have diabetes, you might want to buy it for this very reason. Now wait a minute.
“No sugar added” doesn’t mean that the product is carb-free or calorie-free. It is sometimes being confused with sugar-free; in fact, there’s a bunch of websites that do just that. The problem is that some foods have sugar in them naturally, such as for example, milk or fruit, so anything containing these two can’t be sugar-free. Besides, no sugar added products can still contain additives with high glycemic index such as Maltodextrin.
 Maltodextrin is made of corn, rice, potato starch, or wheat; it’s a common food additive used for expanding the volume of processed food and for increasing its shelf life.
Maltodextrin is made of corn, rice, potato starch, or wheat; it’s a common food additive used for expanding the volume of processed food and for increasing its shelf life.
It has 4 calories per gram which is the same as table sugar. However, maltodextrin has a high glycemic index, almost twice as much as table sugar does. GI of maltodextrin is 110, compared to 65 of table sugar. This means that it can raise the blood sugar levels very quickly. Per FDA, Maltodextrin has to be listed in the nutrition panel as what it is, a carbohydrate.
4. Sugar-free
This doesn’t automatically mean fewer calories; in fact, sugar-free products still have some sugar in them. By FDA definition, sugar-free foods can have less than 0.5 grams of sugar per serving. They however still have calories and carbs from other sources. One of such sources are sugar alcohols that taste just as sweet as sugar while having half the calories.
Most sugar alcohols have no effect on blood sugar. Some of them however are actually carbohydrates that are well absorbed by the body and can cause blood sugar spikes such as Maltitol. Sugar alcohols can also act as a laxative so keep that in mind when indulging.
Sugar-free products can also have artificial sweeteners that don’t affect blood sugar directly but can affect insulin sensitivity nevertheless.
When I was first diagnosed with diabetes, I started buying sugar-free products thinking that I was doing the right thing. One of the first such products was sugar-free pancake syrup that tasted as sweet as its sugar-containing counterpart. For a brief while I was proud of myself for being able to find a product that is sugar-free and just as sweet. This however was short lived when I had a seemingly unexplained blood sugar spike after eating hot cereal with ‘sugar-free’ syrup. I then took a close look at the Nutrition Panel and low and behold, it listed a few carbs including Sorbitol, a sugar alcohol; corn syrup and molasses. All of the above are carbs.
After having contacted my nutritionist, I was advised to stay away from everything that ends with ‘ol’ (sugar alcohols). From now on, I will never take the statement ‘sugar-free’ for granted but will read the labels first and then decide. A lesson learned.
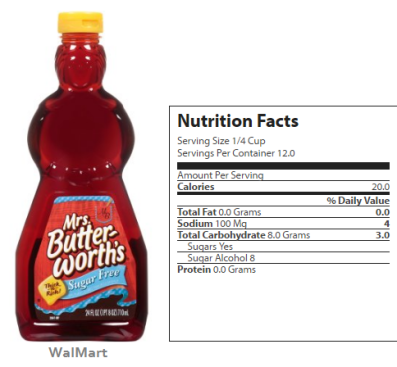
Here now, a bottle of pancake syrup; didn’t the label say “sugar-free”? Yes, it did but the Nutrition Facts panel states Sugars – Yes, and the amount of 8 grams. This is per serving size that mind you, is a quarter of a cup.
Most if not all of us consume a few times over this in one sitting. No, really. A quarter of a cup is a little bitty thing. Most folks will use at least a cupful of it. Then all the seemingly ‘healthy’ content goes out the window.
Ever seen a commercial with a pile of pancakes buried under a huge mound of syrup? There goes your serving size.
5. Low-fat or fat-free
Many of us associate zero trans fat or fat-free claims with healthy, which is exactly the outcome the food manufacturers are trying to achieve. And the truth is, while some foods are naturally low in fat, such as fruits and vegetables, processed food is another story. Fat-free versions of food replace fat with sugar which is no better and eventually gets stored in your body as fat anyway. The keywords to look for are corn syrup and fructose.
Fat-free products are loaded with sugar, and sugar-free are loaded with fat. Here you have it, a no-win situation.
Nutritionpedia website has posted these two labels side-by-side, one is regular, the other, fat-free.

As you can see, the fat-free product contains about three-fold more sugar than the regular version of the same product. Not only would one serving size of the fat-free food have more calories than the full-fat version but you may be tempted to eat two servings because it comes across as healthy.
By FDA standards, low fat means less than 3 grams of fat per serving size and fat-free, less than 0.5 grams. How much is the serving size? This is what the food manufacturers are playing with. One vs two cookies as a serving size or slices of bread likewise, can make all the difference. And who is eating only one cookie? When you or your kids eat more than one, all that low fat content per serving size goes out the window.
THE BOTTOM LINE: sugar-free products are loaded with fat, and fat-free, with sugar. To make sure that you are in fact eating healthy food, you need to do your homework. Check the label of a fat-free or sugar-free product and compare it with the full-fat or full-sugar version. This of course will take some time.
















 This recipe is from Low Carb Store and was invented by Leoni, their resident dietician.
This recipe is from Low Carb Store and was invented by Leoni, their resident dietician.





