
New Year’s resolutions? Pah! One, you can makes changes any time you want, and two, most of us see them as miserable—the lose weight, take up punitive exercise regimes kind. In this part of the world, January is a challenging month. The weather’s dreich, the nights are long and the pennies few and far between. Who wants to add starvation and exhaustion to the mix?
One resolution I do intend to stick to is my campaign to Make Sundays Special again. Years ago, my husband and I used to make a point of doing something on Sundays. He works most Saturdays, so the Sundays were the one day a week we could visit castles, go to Edinburgh, take the motorbike out for a spin, bike to Balloch, drink too much and cycle back via the main road while piddled*. Last year, we fell into the habit of doing nothing. He’d be downstairs catching up on Colombo (why, why, why?), and I’d hide away upstairs working or writing. We added doing the supermarket shopping to a Sunday. As I love food, I don’t mind the supermarket shop but does it belong on a precious day off? I think not.
Cut the screen time
In 2019, I’ve vowed to spend less time in front of a screen. I’m there for work and as a hobby, and I dread to think how many hours I spend hunched over my laptop. On the plus side, I use a standing desk so it’s not as sedentary as it could be. On the other hand, it’s still not healthy. Time to reinstate the Sunday activities, such as:
Ben Lomond
I have Ben Lomond in my sights. Hill climbing is one of the best activities you can do in Scotland. The Munro is right on my doorstep, and the shame is I’ve yet to climb it.
Three Lochs Walk
I’d also like to walk from Balloch to Helensburgh with Sandy. I’ve done it a couple of times with my friends, and it’s a fabulous walk because of the views you get of Loch Lomond.
Linlithgow Palace
We’re members of Historic Scotland and we’ve yet to visit Linlithgow Palace so a train trip there and a pub lunch is in order.
Uni tour
The University of Glasgow offers walking tours. As I work there, it will be fascinating to find out more about this iconic Glasgow building. Another tour that has always piqued my interest is the one you can do of Glasgow Central station. If I book now, we might get there in the summer. (It’s terrifically popular.)
Sunday roast

Finally, it’s nice to include special meals in your Sunday plans. As a child, I didn’t like the Sunday roast—probably because it meant sitting at the table waiting for adults to finish so we children could be excused, and I have memories of thick slabs of meat and nasty bits of under-cooked fat. These days, I’m a fully paid up member of the Sunday roast forever club. While the meat is nice, the best bits are the accompaniments – home-made gravy with a decent amount of wine thrown in, roasted parsnips and carrots, crackling if you’re making pork (or just make it as a side dish anyway) and one roast potato as a treat.
Bring on the special Sundays!
What’s your idea of a treat on a Sunday? Is cutting back your time online part of your plans for 2019, and if so what do you intend to do instead?
*Don’t do this at home, folks!


 You find me, un-sensored and sad… Yes, I’ve completed two weeks on the FreeStyle Libre sensor and reader system, and now I’m back to finger pricks, at least temporarily.
You find me, un-sensored and sad… Yes, I’ve completed two weeks on the FreeStyle Libre sensor and reader system, and now I’m back to finger pricks, at least temporarily. A continuous glucose monitoring system, the MiniMed 670G self-adjusting insulin pump, a personal trainer AND an unlimited food budget so I can buy organic, ethically sourced food all the time…
A continuous glucose monitoring system, the MiniMed 670G self-adjusting insulin pump, a personal trainer AND an unlimited food budget so I can buy organic, ethically sourced food all the time…
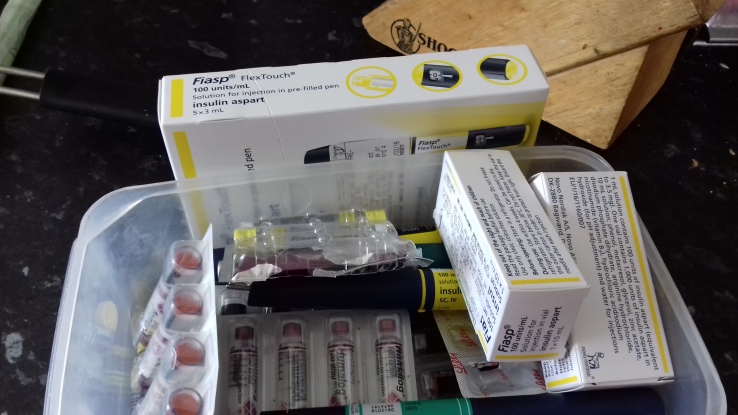 Insulin shortages and low-carb dishes—no obvious connection, I grant you but bear with me.
Insulin shortages and low-carb dishes—no obvious connection, I grant you but bear with me.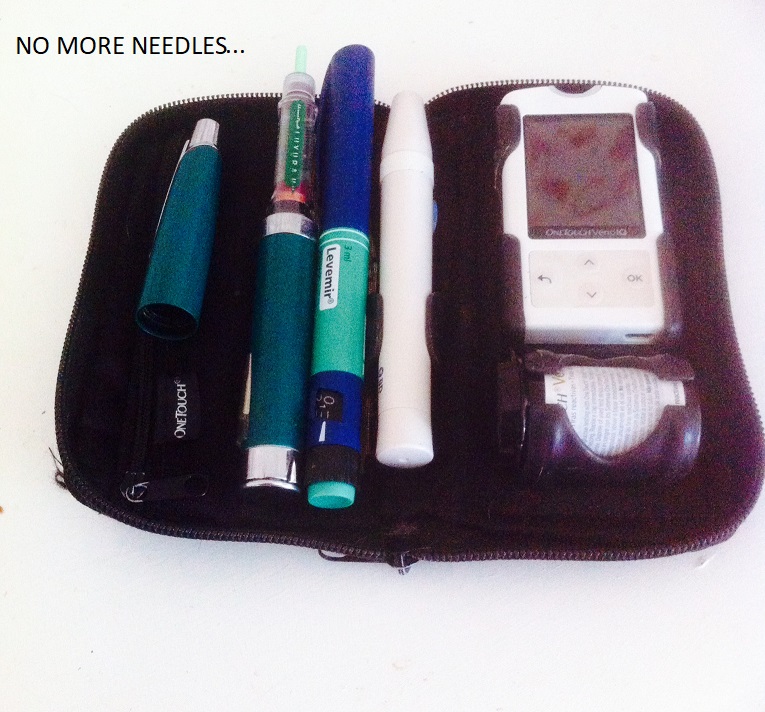
 Google alerts frequently pairs ‘diabetes’ and ‘cure’ together, but most of the time the words don’t capture my attention. Even when ‘type 1 diabetes’ and ‘cure’ make the same sub-heading, I’m not jumping up and down.
Google alerts frequently pairs ‘diabetes’ and ‘cure’ together, but most of the time the words don’t capture my attention. Even when ‘type 1 diabetes’ and ‘cure’ make the same sub-heading, I’m not jumping up and down.
