The vote to take the UK out of the EU has chilled me to the bone. Social well-being is inextricably linked to health and a careless decision taken by a majority of around 52% of voters has just messed up our economic system on which our well-being as citizens and patients depends.
Scotland, Northern Ireland, central London and Gibraltar have unequivocally voted to stay in the EU. There are 1.3 million Brits who study, work or have retired to the EU, and many of these people were not able to vote in the referendum. If they had, the margin of success for Brexit would have been lessened considerably.
The people who voted to stay tended to be younger, have degrees, have jobs, and be wealthier. Those who wanted to leave tended to be older, be on benefits and perhaps feel that they will be more sheltered from the effects of their choice.
Economists, business leaders, bankers, most MPs, and the British Medical Association which represents the majority of UK doctors, all want to stay in the EU. Reasoned discussion has been going on for months in such papers as the Guardian and the Times. Pictures of the Union Jack, the Queen, and rants about immigration and the millions that could be diverted to the NHS have been on the front pages of the tabloids for months. On the very morning of the result, Mr Farage, leader of the UKIP party, admitted that the slogans on the buses and billboards about money going to the NHS from the EU were lies. “Nothing to do with me”, he said.
Meanwhile the UK has lost David Cameron as Prime Minister. He has been an emotionally stable, sensible, well informed, inclusive, solution seeking head of the government. Very far from Maggie Thatcher or Tony Blair in performance or nature, he has felt the need to step down, despite demonstrating an integrity that Farage and the likes do not appear to emulate.

So, what has the EU done for us? Quite a lot as far as I can see. Most of it beneficial.
We have a decimal currency, much easier than the old 12 unit system. We get cheap good quality food, particularly fruit, vegetables, wine, ham, olive oil, nuts and cheese. Many of these items feature heavily in a low carbohydrate Mediteranean style diet which is so important in keeping well if you have diabetes.
For doctors, the European Working Time Directive, which limits junior hospital doctors working hours to 48 hours a week was a God send. I used to work 120-145 hours a week as a junior doctor. It was described as “training” but it was slave labour. I was paid one third of my basic rate for the extra hundred or so hours I was on evenings and weekends. On Christmas day 1983 I earned 50 pence per hour and that was before tax. Older doctors and consultants didn’t care. They did nothing about it. If we did it and survived, you can too was the mentality. It took the EU to get doctors out of that mess and without the working directive it could easily revert back.
There is a workforce crisis in UK medicine as it is. Worsening of terms and conditions for doctors will lead even more of them to jack it in and head for Australia.
What of our working population generally? The EU have brought in laws to give reasonable hours, breaks, holidays and contracts to workers. Without the EU there will be more likelihood for zero hour contracts to become the norm, if you can even get a job.
When it comes to selling a house, the main thing that estate agents say are important are location, location, location. When it comes to the well -being of a countries citizens the important things are economy, economy, economy.
Like it or lump it, we are all part of a global economy now. The EU is not responsible for all the bad things that are happening that affect the economy. The immigration crisis is due to an undeclared third world war which is due to Islamic separatists destroying these people’s homes, countries and own economies.
A government can’t hand out money to sick people, the unemployed, the NHS or anyone else unless they have money raised from taxation. They can’t get this unless people have jobs. If the economists are right, and there is no reason to believe that they will not be, there will be fewer jobs, worse terms and conditions, less money able to be raised from tax and therefore less money for pensions, benefits and health care.
Leaving the EU is not a vote for prosperity.
What can we do about it?
To really improve things we need to get a review of the referendum decision. If it can’t happen for the whole of the UK, the best option in my view, then perhaps it can be achieved in Scotland. This would mean a difficult choice for Scots. Do we stay with England and Wales? Do we stay with Europe?
When people look across at Southern Ireland it would appear that they have not done very well in terms of economic prosperity by staying in the EU. On the other hand do we revert back to the dark ages with the working classes being over worked and underpaid with a deficient social care system but with an elite few at the top as could happen for England and Wales?
What do you think of the result of the vote? What do you think we can do to makes things less awful than what has been predicted for us all?
Dr Katharine Morrison
 As of today, the UK has a new prime minister – Theresa May.
As of today, the UK has a new prime minister – Theresa May.
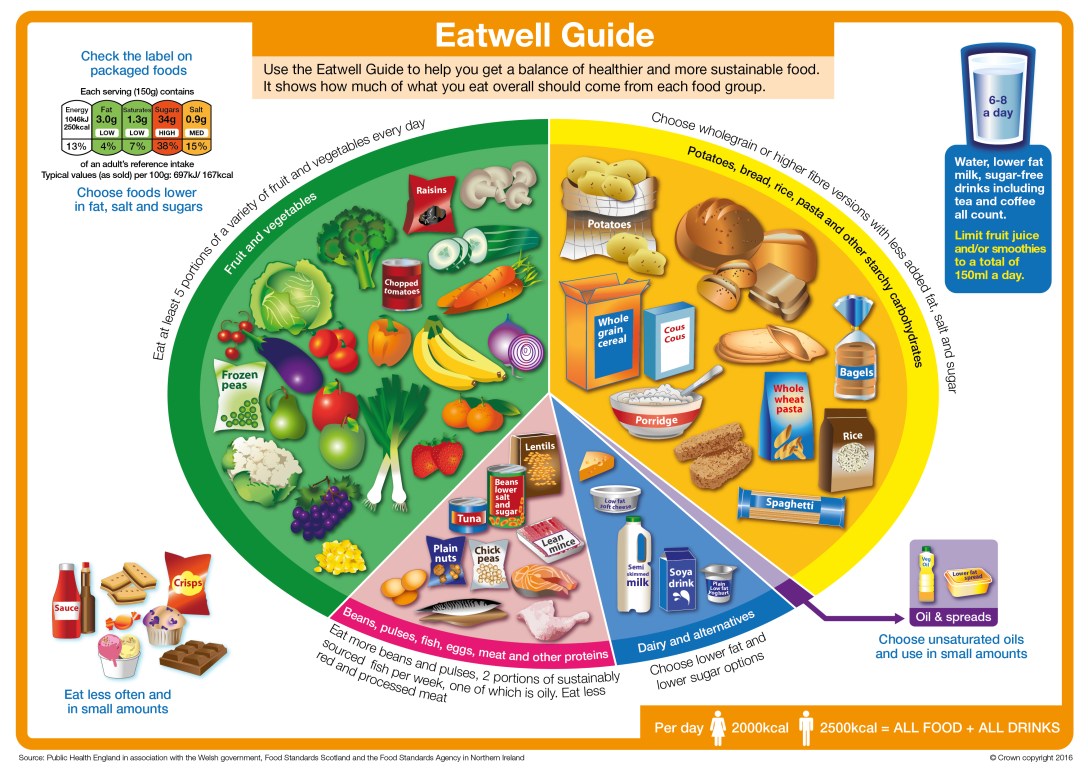
 They have said that 150g of fruit juice or smoothie can count as one of “your five a day”.
They have said that 150g of fruit juice or smoothie can count as one of “your five a day”.





 In the UK 25% of adults are obese, the highest prevalence in Europe, and type 2 diabetes has risen by 65% in the past 10 years with no sign of slowing down. Together they cost the NHS £16 billion a year and the UK economy at large £47 billion a year.
In the UK 25% of adults are obese, the highest prevalence in Europe, and type 2 diabetes has risen by 65% in the past 10 years with no sign of slowing down. Together they cost the NHS £16 billion a year and the UK economy at large £47 billion a year.



