

|
The best diet for optimal blood sugar control & health
|

As reported in Naturally Healthy News Issue 24
Eating a diet that’s rich in carbohydrates – sweets, soft drinks, bread, pasta and potatoes- is a direct cause of mild dementia and memory loss as we get older. Starch and sugar cause cognitive impairment.
A diet that is high in fats and protein is far less likely to cause mental decline, say Mayo Clinic researchers.
They have found that carbohydrates interfere with the body’s ability to metabolise glucose and insulin which are needed to feed the brain.
The carbohydrate link was found when researchers analysed the lifestyles and diets of 937 people aged 70-89 years. They found that those who ate the most carbohydrates were 3.6 times more likely to show mild cognitive decline, including problems with memory, language, thinking and judgement.
Those who ate fats were 42% less likely to suffer cognitive decline and those who ate high protein diets had 21% less risk.
( Alzheimers Dis, 2012;32:329-39)
Great recipe for low-carb crackers.

So, can I be frank with you? Getting enough fiber in a low carb keto diet can prove to be a bit challenging at times. Sure, there are supplements you can take to ensure your fiber levels are high enough, but why? If I’m given the option of taking a fiber supplement or a a tasty snack, what do you think I’m going to choose?
This foodie wanted to create a delicious low carb high fiber cracker. I know there are plenty of good recipes out there for low carb crackers, but I not only wanted a delicious cracker, I wanted it to meet my fiber needs too. Can I hear an amen from those who’ve been wanting the same thing?
I must admit that at times I crave regular wheat crackers but a high carb, gluten-loaded cracker is the last thing I need. Which is why I just let…
View original post 603 more words

In part two of Dr Lardinois’ interview for Diabetes in Control we learn more often overlooked points regarding albumin.
 In part 2 of this exclusive interview from AACE 2016, Dr. Claude Lardinois discusses why albumin is a driver of cardiovascular disease.
In part 2 of this exclusive interview from AACE 2016, Dr. Claude Lardinois discusses why albumin is a driver of cardiovascular disease.
Steve Freed: I woke up with a nightmare and I said to myself (and it goes to what you’ve been saying) microalbumin in the urine can actually be an indicator for heart disease, diabetes, and kidney failure.
Dr. Lardinois: And congestive heart failure too.
Steve Freed: I was told by a doctor that 10% of the population has some form of kidney issues and that if we prevent one person from going on dialysis, that’s a quarter of a million dollars over their lifetime. Just one person. I said to myself. Well, wait a second, we have microalbumin tests right now. I looked into it and you can perform a microalbumin test with blood, you can also do a dip stick in your office. But there is no FDA approved test for home use to detect microalbumin. Now if you remember, we had colon cancer tests where you put a piece of feces in the mail, and we found all these people and we saved millions and millions of dollars.
Dr. Lardinois: I would say two things: one is, I would discontinue using the term microalbumin. Now the reason I say that is I’ve actually asked students or residents what microalbumin is, and do you know what they think it is? It’s a smaller molecule of albumin. It’s a small albumin molecule. There’s a small albumin and a big albumin. Well, there’s not! It’s just albumin, period.
Steve Freed: So I said to myself, let me investigate this. So I went out and I found overseas a test that’s like a pregnancy test. A plastic container, put two drops of urine in it. If the red line comes up, you’ve got “albumin” in the urine. Obviously if you’re lifting weights, you might have albumin in the urine. If you have a cold, you might have albumin in your urine. So I asked the doctor, he said you know I tried this about 20 years ago, and what they discovered was it was too costly. Well, I found a way to get this thing made for less than a dollar. It has to get FDA approved. My thought is you can send these out and I would send two, maybe even three tests out, and if one was positive, you do another one in a week and if that was positive, you can do another one. If you get two positives then you need to contact your physician and have them do further testing. Because you could be at risk. I know I can’t say that you’re diagnosed. All I can say is you’re at risk and more tests have to be done and you need to contact your physician. Send this out to the self-insured companies that have 10,000 employees, send it out with your tax refund, if the check is no good.
Dr. Lardinois: I’ll share with you, I’ve got a couple of very important things. You said something about nightmares though?
Steve Freed: Well I had a nightmare because of all these people I have to talk to, this doctor and I said a quarter of a million dollars.
Dr. Lardinois: You don’t have diabetes do you?
Steve Freed: No, it’s in my family.
Dr. Lardinois: Because what I tell you is that I tell people that a nightmare or a bad dream is a hypoglycemic reaction. When you said that, I used to do camps for kids and there were kids that would have a 400 blood sugar in the morning and everybody thought they didn’t take their insulin. They had too much insulin and they rebounded. Here’s the issue with albumin…. Albumin in the urine. What do they tell you your albumin in the urine should be? Less than 30. Where did that number come from?
Steve Freed: The albumin test is greater than 20.
Dr. Lardinois: That’s because you have to correct for grams of protein so it actually becomes 30. It’s 20 mg but when you correct for creatinine it’s actually 30. That number of 30 was generated by the nephrologists. What they showed was that if you had less than 30 mg of albumin in your urine, your chances of going onto end stage renal disease was zero, almost zero. If you had between 30 and 300, that’s where they came up with the term microalbumin. It really wasn’t microalbumin, it was just albumin in the 30 to 300 range. You had a small percentage of going into end stage renal disease. If you had more than 300 in your urine, I tell my patients, you better start learning the word nephrologist. Not endocrinologist, because you’re going to do that. But I can tell you, the true value, the goal for albumin in the urine is 7.5 in women and 4 in men.
Steve Freed: You say 4 and 7, what does that mean?
Dr. Lardinois: I’m saying instead of 30 it should be 7.5 for you [Joy], and 4 for you [Steve]. There are studies now, and I will show this data, that once your albumin in the urine is more than 5 mg per gram of creatinine, your mortality starts to go up. When you get to 30, you’ve already doubled your mortality. So you’re twice as likely to die if you have a 30 as a 5, but everybody says it’s normal because you’re less than 30. The other thing they don’t take into account, but I’ve learned from a couple nephrologists here, that they actually are addressing now is you [Steve] versus her, because you have a bigger muscle mass than she does. You’re going to have a seriously lower creatinine because it’s an albumin to creatinine ratio, because you have a bigger creatinine, your numbers actually are going to be lower. But when you correct it for lean body mass, your numbers should be lower, so yours should be 4 and hers is 7.5. But I’m going to do a whole hour on that.
Steve Freed: So what do you think of that? I’ve already got a lab, we’re working on it, we’re putting it together, we’re putting together a business plan to develop this and get it FDA approved.
Dr. Lardinois: I think it would be a great idea, but I’m hoping that the FDA and that societies will stop looking at 30 as the normal.
Steve Freed: Where can I get this information?
Dr. Lardinois: Which information?
Steve Freed: That 30 is not normal.
Dr. Lardinois: I can give you all the information you want. I can send you the talk I gave in Hawaii and it’s going to be similar in December, but obviously I’ve got some new information just in the last couple weeks. I always update my presentations.
Steve Freed: I’d like to transcribe it so I can hand it to the National Kidney Foundation.
Dr. Lardinois: I’ve been very adamant. I’ve not got anywhere with it. Even some of them say, what are you talking about, let’s do a physician paper. I said ok fine, but your blood pressure, lipids, continuous glucose monitoring. Why don’t you actually do one on albumin? In fact I even said I would be happy to even chair it, if you were willing to do it, because I think it’s something that’s really important. The problem with albumin right now, is we’ve never designed any good control studies, so all the data we have is observational. Observational studies, that’s the problem with nutrition. All of them are observational studies, and that’s been flawed. So that’s prevented us. Until the FDA will accept albumin as a legitimate marker, and say, ok, we must get below 7.5 in you, we must get below 4 in you, let’s see what happens? I’ll guarantee you, I’m from Nevada but I don’t spend money at the casinos, but I would [spend] some serious money on that. I’ll bet you, I’ll bet $25,000 that if you did a clinical study and you got it below 7.5 in women and 4 in men, you would save a lot of lives.
Steve Freed: That’s going to take time to show.
Dr. Lardinois: Exactly, but they’ve got studies where they’ve done it, but they didn’t want it. It wasn’t part of the end point. But they’ve got studies like Life study which shows normal albuminuria and the death rates up 200% with a “normal” albuminuria. I’ll be happy to send you that.
Diabetes in Control will continue to provide updates as more information becomes available.
Claude K. Lardinois, M.D., FACP, FACE, MACN, is a professor of medicine at the University of Nevada School of Medicine and a member of the graduate faculty for Nevada Studies in Nutrition at the University of Nevada, Reno.
Portions of this interview transcript have been edited for brevity and clarity.

What To Cook In January | jovinacooksitalian

This is a hearty entree and only needs one vegetable as a side. flounder comes in large sizes here on the gulf and mine weighed 14 oz. Substitute an equal amount of smaller fillets. If you can’t get flounder this recipe works well with any flat white fishfillet eg sole.
For 2-3
Ingredients
Crab Filling
1 tablespoon each of minced onion, celery and bell pepper
2 tablespoons mayonnaise
1 tablespoon Dijon mustard
¼ teaspoon seafood seasoning (Old Bay)
1/2 pound lump crab meat
Flounder
12-14 oz flounder fillet or fillets
Paprika
Chopped fresh parsley
Directions
In a small bowl, combine all the filling ingredients, except the crab. Then, gently fold in the crab. Place the flounder in a baking dish coated with olive oil.

Spoon the crab mixture evenly over the fillet or fillets. Sprinkle with paprika and parsley.
Bake at 400°F for 20-24 minutes or until the fish is cooked through.

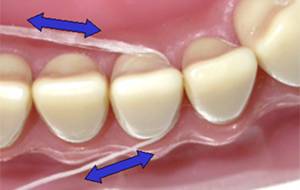
Researchers in the Athlone Institute of Technology in Dublin Ireland have been researching the effects on coconut oil on oral health. They have found that coconut oil kills most bacteria in the mouth and importantly the ones that cause tooth decay. The oil is also effective against Candida Albicans that causes thrush.
The team think that it should be added to commercial toothpastes. Indeed there are some makes available. You can also make it yourself. One recipe has coconut oil, baking soda and peppermint oil.
As poor dental health, gingivitis and thrush do affect diabetics more severely than many people perhaps this new finding can help.
(Reported in Naturally Healthy Issue 24 www/ait.ie/aboutaitandathlone/newsevents/pressreleases/2012pressreleases/title-16701-en.html)
 Omega 3 fatty acids may help in the treatment of type 1 diabetes, according to a recent article in the news.
Omega 3 fatty acids may help in the treatment of type 1 diabetes, according to a recent article in the news.
Medical News Today reported that new research published in The Journal of Clinical Investigation showed Omega 3s reduced the auto-immune responses typical of type 1 diabetes, and that supplementation could treat and even reverse autoimmunity in type 1 diabetes.
Researchers, led by Allan Zhao at the Guangdong University of Technology, China, added Omega 3 fatty acids to the diet of non-obese mice with type 1 diabetes. They also increased the levels of Omega 3s in the mice through genetic modification.
The mice were tested every three months for glucose and insulin tolerance. The examined the pancreas of the mice for insulitis—an infiltration of lymphocytes in the islets of the pancreas, a phenomenon typical of type 1 diabetes. They collected blood from the mice and measured their levels of serum insulin.
The study found that adding Omega 3s to the diet significantly improved the metabolism o glucose and decreased the incidence of type 1 diabetes in the mice.
There was a decrease in pro-inflammatory cell-signalling protein and a considerable drop in insulitis. Zhao and his team also noticed signs of beta cell regeneration in mice that had been treated with Omega 3s.
Supplementation AND genetic therapy normalised blood sugars and insulin levels for a minimum of 182 days.
The researchers concluded that their observations “may offer clinical guidance” to people who were at the early onstage of type 1 diabetes*, or who have consistently sound management of their blood glucose levels.
There are a lot of stages from animal tests to prescribed treatment for humans. In the meantime, can we recommend adding in plenty of oily fish to your diet? It won’t do any harm. Here are some of our favourite fishy recipes:
If you buy grass-fed beef, and eggs from free-range hens that are fed a diet high in Omega 3s, you can get your nutrients that way too.
*Sigh. It’s always the newbies, isn’t it?!

This is a two part interview with Professor of Internal Medicine Dr Claude Lardinois given to Diabetes in Control. We learn new things from him that are not emphasised enough in the medical community.
Continued smoking is THE factor that causes the most amputations in diabetics.
Feet should be examined EVERY time a diabetic sees a health care professional.
Diabetes = cardiovascular disease due to insulin resistance + high blood sugars
Apart from blood pressure and cholesterol, urinary albumin and genetic tests can help individualise the advice and treatment that is given to patients.
P E N T A D is a memory aid for doctors when they see a diabetic: protein in the urine, eyes, e, necklace, toes, A1C, document.
The Impact of Genetics in Cardiovascular Disease
In part 1 of this exclusive interview from AACE 2016, Dr. Claude Lardinois discusses amputations and SGLT-2s, and genetic risk factors for cardiovascular issues in diabetes patients.
I think smoking is a huge factor in amputations. In fact, I personally think that in my practice anyway, 90% of the patients that have amputations are the ones that continue to smoke.
Joy Pape: So, how do you teach your patients about foot care and preventing amputations?
Dr. Lardinois: We have a policy that you have to get your shoes and socks off immediately when you get in the room.So we inspect the feet every time we see the patients. When I have patients that are smokers, I look at their leg and I’m checking for sensory and that and I say, do you like your legs?
Well of course, Dr. Lardinois, I like my legs. Well if you keep smoking, you’re not going to have your legs. I say, do you know what a black and decker is? Well yeah. We might as well do a black and decker right now. Because that’s what’s going to end up happening if you keep smoking.
I’m amazed because I’ve actually had patients that have quit smoking. I just saw one of my patients not too long ago, and the nurse said your black and decker’s here today. She laughed, she said you got me to quit smoking, because you emphasized to me the importance of my legs.
Joy Pape: This could be very interesting. You might come up with some very interesting ways of getting people motivated to manage their diabetes better. Something else we were talking about earlier [was] about cardiovascular disease. Or just managing diabetes and the topic of genetics. Tell me more.
Dr. Lardinois: Let’s talk about diabetes and cardiovascular disease, because if you look at patients with diabetes and patients without diabetes, the only difference is one has an elevated blood sugar, the other does not.
So, intuitively, the thought process was, particularly from the ADA, is if you lower the glucose to normal, your heart disease will go away. Doesn’t happen. You still have heart disease, because it turns out it’s not the glucose, it’s that you have insulin resistance.
I’ve been accused by my colleagues that I’m really not an endocrinologist, I’m a cardiologist disguised as an endocrinologist, because I really don’t get too hung up about the blood sugar. I don’t have to have it 6.5 or 7. I tell my patients, you are going to die of heart disease.
So what are the factors that make the most difference in cardiovascular disease?
Blood pressure. I’m a very big believer in blood pressure control. Lower is better. Again, you have to be careful in some elderly patients.
But cholesterol is very important, measuring albumin in your urine is very important. So these are all factors, but even after we do that, we’re still evaluating people as a group, not as an individual. That’s where the genetics come in.
There are certain genetic tests that everybody should have done, whether you have diabetes or not. Some of those are Apo-E [tests].
Apo-E is a very important gene that really determines what type of nutritional recommendations you’re going to make for your patient. If you’re a 2-2 or a 2-3, or if you’re a 3-3 or a 3-4, it’s going to vary on what the nutritional recommendations are.
Another thing is, we always talk about alcohol as being good for you — modest alcohol consumption. If you’re an Apo-E 4 and 25% of the population has either 3-4 or 4-4, alcohol actually makes your cholesterol worse and it increases cancer, particularly breast cancer in women. Some of my colleagues say I’m not going to measure my Apo-E 4, because I like alcohol. You’re going to tell me I can’t drink anymore. But we have to explain to those patients that they really have to limit their alcohol to one drink a day. So that’s very important nutritional information, right from the start, that you would never get by just following the standard guidelines.
There’s other genetic markers. There’s actually a statin marker — a lot of controversy behind it. But I stand firm that there’s a certain gene that we have called KIF6, and if you don’t have the variant, the studies with two of the cholesterol drugs weren’t very compelling, that they lowered LDL, but they didn’t reduce heart disease. So I tell a lot, if you don’t know what your KIF6 variant is, which most doctors don’t (I know mine), you have to be very discretionary in which statin you prescribe.
Then there’s other genes that you could also look at. One is haptoglobin; haptoglobin is how we carry our oxygen around. It turns out that there’s three different haptoglobins, 1-1, 1-2, and 2-2. Well, patients with type 2 diabetes who have 2-2, have a 45 percent increased cardiovascular event rate.
So again, that’s why I think with cardiology, we have these studies, even if we aggressively treat their lipids, we still have this 30% residual. Well, I don’t think that residual is cholesterol. I think it’s haptoglobin, APO-E, maybe the statin that you’re prescribing; other factors, albumin in the urine.
I think albumin in the urine is a powerful risk factor for heart disease. But unfortunately the FDA doesn’t see it as a good primary endpoint. I think until they do that, and actually establish a primary endpoint for that, we will never get a valuable answer. There’s no question about albumin in the urine. People think it’s just the kidney, albumin in the urine is the kidney telling you, you have endothelial disease. That you are leaking albumin throughout your entire body. That albumin drives cardiovascular disease. Big time.
Joy Pape: So, do you refer your patients for genetic counseling? If this is the way you practice, how do you learn more about their profile?
Dr. Lardinois: Right now it’s been kind of challenging. The diabetes [practice] I was in, they were not all that receptive. Change is always hard to do. So I actually worked with two of my former medical students, who are now practicing physicians in Reno. There’s a concierge service. I helped them set-up a genetic thing, so if patients do want to come in, they pay cash now. It’s only $1000 for the genetic testing. You do a treadmill which is $1100, and that doesn’t tell me anything. I think treadmills are kind of useless. I went 16 minutes on the treadmill, and I’ve got heart disease. I went 16 minutes. Well they’d tell me I’m just fine. Well, I’d be dead now. That’s what happened to the guy on Meet the Press. He had a treadmill [test] and three days later he was dead. What was his name? I’ll think of it in a second. [ed. note: Tim Russert.] Right now, it’s been hard to get it implemented, and I’m moving to a different position in a different hospital and maybe I can get involved with a cardiologist and get this up and running. I do think there’s basic genetic testing that should be implemented in the management of everybody with any disease, and it’s not that expensive.
Joy Pape: So we talk about patient education and people making changes. Behavior change. So how did it work? How does it work if your patients find they have this certain gene and they need to cut down on their drinking? Have you had any experience with that?
Dr. Lardinois: Oh yeah, some of them aren’t really happy with that. But I say, I provide you a service. I’m not your mom or your dad and I provide you a service and I say based on this information, you should reduce your alcohol consumption to one drink a week.
Joy Pape: Is it effective?
Dr. Lardinois: In some people it is. I think 70% of patients will follow along with you, but I think 30% no matter what you do [won’t]. There’s patients that I say [to], I feel sorry, I feel bad today. They say why? You came in, I gave you these recommendations three months ago, you didn’t do any of them. Your A1C, your blood pressure, your cholesterol, your kidney test is all the same. I’m going to have to charge you $75 for this. We live in Nevada, you could go to a nice big buffet with your whole family for $75. So I feel kind of bad, I’m taking their money away because why did they even bother to come? They didn’t do anything.
Joy Pape: Well, I’m sure glad you came today. I think it’s obvious why you got this award that you’ll be getting tonight. So congratulations and thank you.
Dr. Lardinois: Just one other point I’d like to share that I think is important. One of the things I try to do is, I work with the VA to try to set up ways to get doctors to better manage their [patients’] diabetes. I actually came up with this thing called PENTAD. I published it in Archives of Family Medicine. It was very short. Just a little card, a pocket card. The P stood for Proteinuria, which would be albumin. The E stood for Eyes. Make sure you have your patients get their eye exam. N was necklace or bracelet. Make sure they have a bracelet. T was toes, check the toes. The A was A1C. And then you say well it’s PENTAD, you have the D, so what’s the D? I said that you Document in the chart that you did the PENTA. I was very successful. It worked very well. I was going through some old papers of mine and I came up and had a few of my PENTAD cards left that I did. I did camps for kids with diabetes for 18 years and I think Lilly or somebody nicely made these PENTAD cards, so we just gave them out to everybody.
Joy Pape: It’s great to have those memory tags, something to remember.
Dr. Lardinois: We actually had a stamp. We had a stamp at the VA where we just stamped the PENTAD in and you could just write it in. That improved compliance tremendously, because it’s a reminder.
Joy Pape: I know it’s something I’ll use. Thank you so much.

Cooking The Italian Provinces – Rome | jovinacooksitalian

Serves 4
Ingredients
Directions
In a heavy-bottom saucepot, heat the olive oil.
Season the oxtail pieces with salt, browning each side of the pieces. Remove; set aside.
Add the onions and a pinch of salt to the pan. Sweat the onions until they are translucent, about 5 minutes.
Add the carrots, cooking until tender, about 5 minutes. Add the celery and garlic. Cook 3 minutes more.
Add the oxtail pieces back to the pot. Deglaze with the wine over high heat, cooking about 2 minutes.
Add the tomatoes; bring to a boil. Continue boiling to cook off some of the tomato water.
Add the beef stock just to cover the meat, then the pepper and cloves.
Bring to a boil. Once it boils, lower the heat to a simmer, cover with a circle of parchment paper, and cook for 4 hours (stirring occasionally).
Once the oxtail is tender, remove the pieces to a serving dish. Cover with aluminum foil; set aside.
Strain the sauce, pressing down on the vegetables to extract all the juices.
Skim all the fat off the top, and pour into a smaller saucepan. Bring to a boil and cook, reducing by 1/4.
Taste for seasoning. Pour the sauce over the oxtail and serve


The results from a new study show that risk increased in women with an early HbA1c of at least 5.9% regardless of a gestational diabetes diagnosis later in pregnancy.
Risk of obstetric complications increases linearly with rising maternal glycemia. Testing HbA1c is an effective option to detect hyperglycemia, but its association with adverse pregnancy outcomes remains unclear. Emerging data sustains that an early HbA1c≥5.9% could act as a pregnancy risk marker.
The purpose of the study was to determine, in a multi-ethnic cohort, whether an early ≥5.9% HbA1c could be useful to identify women without diabetes mellitus at increased pregnancy risk. Primary outcome was macrosomia. Secondary outcomes were pre-eclampsia, preterm birth and Caesarean section rate.
1,228 pregnancies were included for outcome analysis. Women with HbA1c≥5.9% (n= 48) showed a higher rate of macrosomia (16.7% vs. 5.9%,p= 0.008) and a tendency towards a higher rate of preeclampsia (9.32% vs. 3.9% ,p= 0.092). There were no significant differences in other pregnancy outcomes. After adjusting for potential confounders, an HbA1c≥5.9% was independently associated with a three-fold increased risk of macrosomia (p= 0.028) and preeclampsia (p= 0.036).
They evaluated data on 1,228 pregnant women from April 2013 to September 2015 to determine whether an early HbA1c of at least 5.9% can identify women at increased risk for adverse pregnancy outcomes.
Participants were screened for gestational diabetes at 24 to 28 weeks’ gestation, and HbA1c measurement was added to first antenatal blood tests. The primary outcome of the study was macrosomia, and secondary outcomes included rates of preeclampsia, preterm birth and caesarean section.
Compared with participants with an HbA1c less than 5.9% (n = 48), participants with an HbA1c of at least 5.9% (n = 1,180) were more often members of ethnic minorities, had higher pre-pregnancy BMI, were more likely to have anemia and microcytosis, and were more likely to be diagnosed with gestational diabetes.
The rate of macrosomia was increased nearly threefold in participants with HbA1c of at least 5.9% compared with participants with HbA1c less than 5.9%; there also was an increased tendency toward preeclampsia. The rates of preterm birth and caesarean section did not differ significantly between the two groups.
Among participants with HbA1c of at least 5.9%, 22 were diagnosed and treated for gestational diabetes.
From the results of the study it was concluded that, in a multiethnic population, an early HbA1c ≥5.9% measurement identifies women at high risk for poorer pregnancy outcomes independently of GDM diagnosis later in pregnancy. Further studies are required to establish cutoff points adapted to each ethnic group and to assess whether early detection and treatment are of benefit.
In an earlier study published by the American Diabetes Association (Diabetes Care, 2014) they demonstrated that a simple A1c blood test can uncover hidden type 2 diabetes in expectant mothers. The study found that the A1c test can accurately detect undiagnosed type 2 and prediabetes in pregnant women.
The hemoglobin A1c done early in pregnancy may be a convenient and effective way to identify women with pre-existing type 2 diabetes or who are at greater risk of worse pregnancy outcomes.
In this study, researchers examined the use of an A1c measurement done during the first trimester as a screening tool for pre-existing diabetes. The test was performed on more than 16,000 pregnant women and compared with the results of a 2-hour oral glucose tolerance test (OGTT), which is performed after an overnight fast, and is the gold standard diagnostic test for type 2 diabetes.
The study found that the hemoglobin A1c test was able to identify all the women with pre-existing type 2 diabetes when an A1c cutoff point of 5.9 percent was used, said Dr. Florence Brown from Joslin Diabetes Center in Boston. “In addition, even if women did not have pre-existing diabetes, the A1c cutoff point of 5.9 was able to identify a population of women at greater risk for adverse pregnancy outcomes, including some women with gestational diabetes.”
This is an important finding because 5.9 percent is considerably lower than the value of 6.5 percent currently used to diagnose patients with type 2 diabetes who are not pregnant, she adds. The 6.5 percent threshold would have missed almost half of these women and is therefore too high for screening purposes, the study authors conclude.
This study also found that an early pregnancy A1c of 5.9 percent to 6.4 percent was associated with a greater risk of worse pregnancy outcomes, including birth defects, preeclampsia and perinatal death.
Given that the prevalence of type 2 diabetes is increasing, the A1c test done as early as possible could identify women at high risk and improve pregnancy outcomes. “This study supports the use of an A1c test in the first trimester and ideally with the first prenatal visit as one possible screen for pregnant women,” said Dr. Brown.
Practice Pearls:
Mañé L, et al. J Clin Endocrinol Metab. 2016;doi:10.1210/jc.2016-2581.
