Joint Health Is Critical to Staying Active
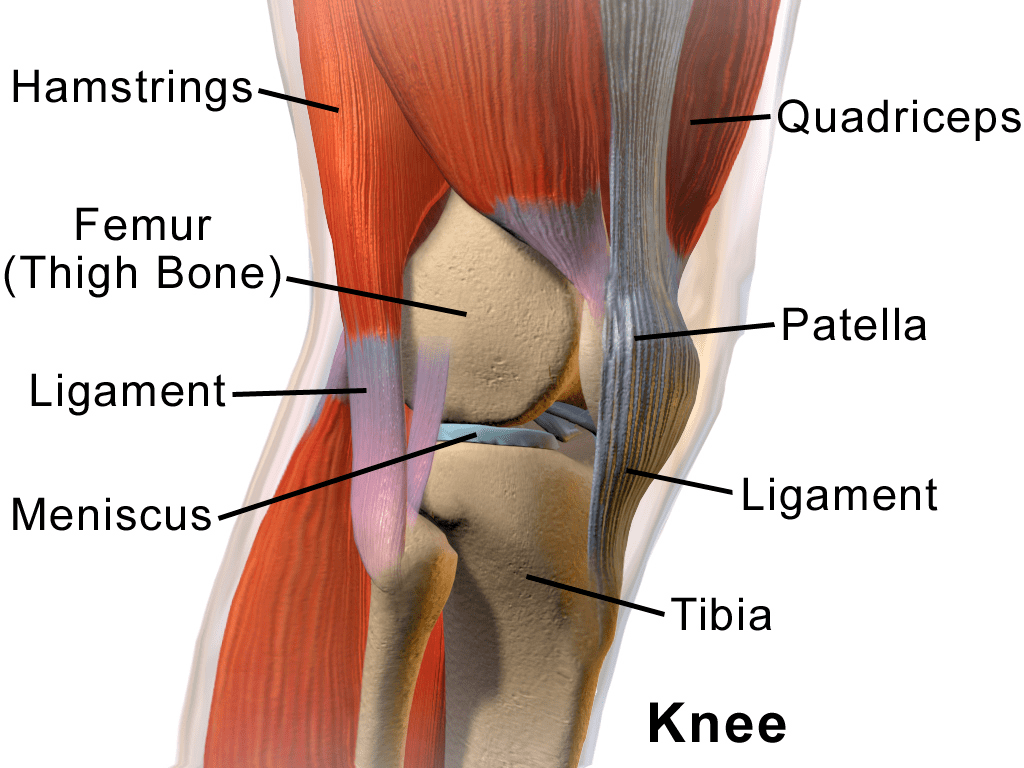
Without properly functioning joints, our bodies would be unable to bend, flex, or even move. A joint is wherever two bones come together, held in place by tendons that cross the joint and attach muscles to a bone on the other side and ligaments that attach to bones on both sides of the joint to stabilize it. The ends of the bones are covered with cartilage, a white substance formed by specialized cells called chondrocytes. These cells produce large amounts of an extracellular matrix composed of collagen fibers, proteoglycan, elastin fibers, and water. Tendons and ligaments are also made up primarily of collagen.
Joints can be damaged, however, making movement more difficult or painful. Joint cartilage can be damaged by acute injuries (i.e., ankle sprain, tendon or ligament tears) or overuse (related to repetition of joint movements and wear-and-tear over time). Damage to the thin cartilage layer covering the ends of the bones is not repaired by the body easily or well, mainly because cartilage lacks its own blood supply.
Aging alone can lead to some loss of this articular cartilage layer in knee, hip, and other joints—leading to osteoarthritis and joint pain—but having diabetes also potentially speeds up damage to joint surfaces. Although everyone gets stiffer joints with aging, diabetes accelerates the usual loss of flexibility by changing the structure of collagen in the joints, tendons, and ligaments. In short, glucose “sticking” to joint surfaces and collagen makes people with diabetes more prone to overuse injuries like tendinitis and frozen shoulder (1; 2). It may also take longer for their joint injuries to heal properly, especially if blood glucose levels are not managed effectively. What’s more, having reduced motion around joints increases the likelihood of injuries, falls, and self-imposed physical inactivity due to fear of falling.
Reduced flexibility limits movement around joints, increases the likelihood of orthopedic injuries, and presents a greater risk of joint-related problems often associated with diabetes, such as diabetic frozen shoulder, tendinitis, trigger finger, and carpal tunnel syndrome. These joint issues can come on with no warning and for no apparent reason, even if an individual exercises regularly and moderately, and they may recur more easily as well (3). It is not always just due to diabetes, though, since older adults without diabetes experience inflamed joints more readily than when they were younger.
So what can you do to keep your joints mobile if you’re aging (as we all are) and have diabetes? Regular stretching to keep full motion around joints can help prevent some of these problems, and also include specific resistance exercises that strengthen the muscles surrounding affected joints. Vary activities to stress joints differently each day. Overuse injuries occur following excessive use the same joints and muscle in a similar way over an extended period of weeks or months, or they can result from doing too much too soon.
Doing moderate aerobic activity that is weight-bearing (like walking) will actually improve arthritis pain in hips and knees (4). People can also try non-weight-bearing activities, such as aquatic activities that allow joints to be moved more fluidly. Swimming and aquatic classes (like water aerobics) in either shallow or deep water are both appropriate and challenging activities to improve joint mobility, overall strength, and aerobic fitness. Walking in a pool (with or without a flotation belt around the waist), recumbent stationary cycling, upper-body exercises, seated aerobic workouts, and resistance activities will give you additional options to try.
Finally, managing blood glucose levels effectively is also important to limit changes to collagen structures related to hyperglycemia. Losing excess weight and keeping body weight lower will decrease the risk for excessive stress on joints that can lead to lower body joint osteoarthritis (5). Simply staying as active as possible is also critical to allowing your joints to age well, but remember to rest inflamed joints properly to give them a chance to heal properly. You may have to try some new activities as you age to work around your joint limitations, but a side benefit is that you may find some of them to be enjoyable!
References:
- Abate M, Schiavone C, Pelotti P, Salini V: Limited joint mobility in diabetes and ageing: Recent advances in pathogenesis and therapy. Int J Immunopathol Pharmacol 2011;23:997-1003
- Ranger TA, Wong AM, Cook JL, Gaida JE: Is there an association between tendinopathy and diabetes mellitus? A systematic review with meta-analysis. Br J Sports Med 2015;
- Rozental TD, Zurakowski D, Blazar PE: Trigger finger: Prognostic indicators of recurrence following corticosteroid injection. J Bone Joint Surg Am 2008;90:1665-1672
- Rogers LQ, Macera CA, Hootman JM, Ainsworth BE, Blairi SN: The association between joint stress from physical activity and self-reported osteoarthritis: An analysis of the Cooper Clinic data. Osteoarthritis Cartilage 2002;10:617-622
- Magrans-Courtney T, Wilborn C, Rasmussen C, Ferreira M, Greenwood L, Campbell B, Kerksick CM, Nassar E, Li R, Iosia M, Cooke M, Dugan K, Willoughby D, Soliah L, Kreider RB: Effects of diet type and supplementation of glucosamine, chondroitin, and msm on body composition, functional status, and markers of health in women with knee osteoarthritis initiating a resistance-based exercise and weight loss program. J Int Soc Sports Nutr 2011;8:8
In addition to my educational web site, Diabetes Motion (www.diabetesmotion.com), I also recently founded an academy for fitness and other professionals seeking continuing education enabling them to effectively work with people with diabetes and exercise: Diabetes Motion Academy, accessible at www.dmacademy.com. Please visit those sites and my personal one (www.shericolberg.com) for more useful information about being active with diabetes.



















 Inputs and Outputs
Inputs and Outputs