The Carnivore Diet: Is It Really Healthy?
by Chris Kresser
Published on February 6, 2019
My comment: There has been a lot of publicity about the benefits of an all meat diet, the opposite end of the spectrum from veganism. Dr Jordan Petersen’s daughter has overcome considerable health problems and she puts it down to an all beef diet. In this post Kris shares information, the good and the not so good about such an extreme diet.
The carnivore diet is a hot eating trend, and many people have reported significant benefits from adopting an all-meat diet. But is consuming only meat healthy in the long term? Read on to understand the mechanisms behind the diet, the potential consequences of not eating plant foods, and a few alternatives to going pure carnivore.
Is an all-meat, carnivore diet healthy?
In my recent debate on the Joe Rogan Experience with Dr. Joel Kahn, I touched briefly on the carnivore diet. I’m a huge believer that meat is an essential part of a healthy diet, but eating an all-meat diet is an entirely different subject, and I think we need to be very careful about assuming that an intervention that works well in the short term will also be safe and effective in the long term.
In this article, I’ll discuss the diets of ancestral populations, how the carnivore diet affects the body, my concerns about the potential consequences of such a restrictive diet in the long term, and alternative dietary approaches that might offer the same benefits without having to go pure carnivore.
Are you considering going carnivore? The all-meat diet is trending, but completely dropping plant-based food off your plate could have a significant impact on your health. Check out this article for a breakdown on the strengths and weaknesses of the carnivore diet. #chriskresser
What Is the Carnivore Diet?
The carnivore diet is pretty straightforward: eat only animal foods and stay away from all plant foods. This means that you are primarily getting your energy from protein and fat and are consuming close to zero carbohydrates.
Many people who have adopted the carnivore diet report faster weight loss, improved mental clarity, healthier digestion, and even improved athletic performance. I certainly don’t doubt the anecdotal reports of people that have found remarkable relief from debilitating chronic health problems with this diet. For many of these people, nothing else they had tried worked.
However, when considering the health of a dietary or lifestyle intervention, I’ve long believed that we should look at the big picture: historical evidence from other populations, plausible mechanisms that explain its effect on our bodies, and scientific data regarding outcomes.
Were Any Ancestral Populations Carnivores?
Let’s start with a brief look at the diets of some supposedly “carnivorous” ancestral populations. Indeed, many ancestral groups thrived on large quantities of animal products. However, every single one of these groups also took advantage of plant foods when they were available:
The nomads of Mongolia nourished themselves on meat and dairy products, but also gained nutrients from their consumption of wild onions and garlic, tubers and roots, seeds, and berries. (1)
Gaucho Brazilians consumed mostly beef, but they supplemented their diet with yerba mate, an herbal infusion rich in vitamins, minerals, and phytonutrients. (2)
The Maasai, Rendille, and Samburu from East Africa primarily ate meat, milk, and blood. Young men almost exclusively ate these animal products but also occasionally consumed herbs and tree barks. Women and older men consumed fruit, tubers, and honey. (3)
The Russian Arctic Chukotka subsisted on fish, caribou, and marine animals but always ate them with local roots, leafy greens, berries, or seaweed. (4)
The Sioux of South Dakota ate great amounts of buffalo meat, but they also ate wild fruit, nuts, and seeds that they found as they followed the buffalo herds. (5)
The Canadian Inuit lived primarily on walrus, whale meat, seal, and fish, but they also went to great lengths to forage wild berries, lichens, and sea vegetables. They even fermented some of these plant foods as a way of preserving them. (6)
Every culture we know of that has been studied ate some combination of animal and plant foods. This does not necessarily mean that animal or plant foods are required to remain healthy, but it does speak to the ancestral wisdom of these cultures.
Five Reasons Why the Carnivore Diet Works
When any diet, drug, or other intervention “works,” it’s important to try to understand the mechanism behind it. In the case of the carnivore diet, there are several reasons that might explain the benefits people report.
1. The Carnivore Diet Can Restrict Calories and Mimics Fasting
Ever felt stuffed after you ate a huge steak? Protein is very satiating, meaning it fills you up and sends signals to your brain that you’ve consumed enough food. It’s no surprise that people report not feeling very hungry and start eating less frequently when they adopt an all-meat diet.
Food habituation may also play a role here. When you eat the same thing day after day, your brain doesn’t get as much reward value from food, so you start to eat less food overall—even if the food is usually something you find rewarding, like a big juicy steak.
The ultimate result is unintentional caloric restriction. Caloric restriction sets off a number of changes. When caloric intake drops, the concentration of insulin, insulin-like growth factor 1 (IGF-1), and growth hormone are significantly reduced. This condition triggers autophagy, which literally means “self-eating”—an internal process of cleaning up old cells and repairing damaged ones. Autophagy is also induced during fasting.
This may be why caloric restriction is so effective at reducing inflammation and alleviating symptoms of autoimmune disease. (7) Of course, caloric restriction also results in weight loss. These are arguably the two primary reasons that people seem to be drawn to the carnivore way of eating, but these effects might also be achieved through simple caloric restriction.
2. The Carnivore Diet Is a Low-Residue Diet
“Residue” is essentially undigested food that makes up stool. A low-residue diet is a diet that limits high-fiber foods like whole grains, nuts, seeds, fruits, and vegetables. It is often prescribed for people with inflammatory bowel disease (IBD) or irritable bowel syndrome (IBS) to alleviate symptoms like diarrhea, bloating, gas, and abdominal pain. (8)
Meat is made primarily of protein and fat, which are absorbed high up in the GI tract, leaving little residue leftover to irritate or inflame the gut. In other words, an all-meat diet is effectively a very low-residue diet and gives the gut a rest.
3. The Carnivore Diet Is Often Ketogenic
If you’re eating large amounts of meat but are only eating once or twice a day and adding extra fat to the meat, your diet is likely ketogenic. A ketogenic diet is a high-fat, moderate-protein diet, with:
60 to 70 percent of energy from fat
20 to 30 percent of energy from protein
5 to 10 percent of energy from carbohydrates
While the carnivore diet has no such macronutrient ratios, it’s likely that some of the benefits that come with eating meat alone are due to the body being in a state of ketosis.
Ketogenic diets have been shown to be helpful for a wide variety of conditions, including multiple sclerosis, diabetes, and neurological conditions like Parkinson’s disease and Alzheimer’s. (9, 10)
4. The Carnivore Diet Changes the Gut Microbiota
Switching to an all-meat diet can also rapidly alter the gut microbiota. A 2014 study found that putting healthy human volunteers on an animal-based diet resulted in significant changes to the gut microbiota in less than 48 hours. (11) The animal-based diet increased the abundance of bile-tolerant organisms and decreased the levels of microbes known to metabolize different plant fibers.
The gut microbiota has been linked to virtually every chronic inflammatory disease that has been studied, so it’s no surprise that an intervention that drastically changes the gut microbiota could have significant implications for health. (12)
The Biggest Potential Problem with This Diet: Nutrient Deficiencies
Now that we’ve established some of the mechanisms involved, the big question is: is the carnivore diet safe?
The short answer is that we really don’t know, since there are no long-term studies that have tracked large groups of individuals on carnivore diets for any significant length of time. One of my chief concerns about it is that it lacks several nutrients that are crucial for health.
There are four micronutrients that are especially difficult to obtain on a meat-only diet. Based on a typical carnivore diet and the Dietary Reference Intakes (DRIs) established by the Institute of Medicine, these include:
Vitamin C: An antioxidant that boosts immune cell function and is important for stimulating collagen synthesis
Vitamin E: An antioxidant that prevents the oxidation of lipids and lipoproteins
Vitamin K2: A fat-soluble vitamin that reduces the calcification of blood vessels
Calcium: A mineral required for healthy bones, muscle contraction, and nerve transmission
If dairy is included in the diet, this will cover vitamin K2 and calcium. However, if you don’t like organ meats, the number of potential micronutrient deficiencies increases significantly. In that case, you can add to the list:
Vitamin A: A fat-soluble vitamin important for proper vision and maintaining immune defenses
Folate: A B vitamin important for cell growth, metabolism, and methylation
Manganese: A trace mineral needed for the proper function of the nervous system, collagen formation, and protection against oxidative stress
Magnesium: A mineral that supports more than 300 biochemical reactions, including energy production, DNA repair, and muscle contraction
It’s also important to note that vitamin C is extremely heat sensitive, so only fresh or very gently cooked organ meats will have appreciable amounts.
Many carnivore dieters claim that the nutrient requirements for the general population simply don’t apply to them. Anecdotally, I know of several individuals who have consumed a carnivore diet for three or more years without any overt signs of nutrient deficiencies.
Still, we’re lacking data. Currently, the DRIs are the best we have to go off of, and I don’t think we have enough evidence to unequivocally say that this diet has no risk of producing nutrient deficiencies in the general population.
Should We Be Aiming Higher Than the Daily Recommended Intake?
Even if the carnivore diet were sufficient to prevent outright deficiency, we should also consider metabolic reserve. Metabolic reserve is the capacity of cells, tissues, and organ systems to withstand repeated changes to physiological needs. In other words, it’s having enough nutrients “in the bank” to be able to deal with a major stressor, injury, or environmental exposure. (13) So if an all-meat dieter manages to meet a recommended nutrient intake, it still may not be enough for optimal health.
Other Reasons an All-Meat Diet May Not Be Healthy
It Lacks Beneficial Phytonutrients
Phytonutrients are chemicals that are produced by plants to protect against environmental threats, such as attacks from insects and disease. They can also have major benefits for our health. Curcumin, beta-carotene, quercetin, and resveratrol are all examples of common phytonutrients.
Some proponents of the carnivore diet suggest that phytonutrients are toxic to humans, and that it’s best to eliminate them completely from our diet. However, many of these “toxins” act as acute stressors that actually make us stronger through a process called hormesis.
Much like resistance training is an acute stressor that leads our muscles to adapt and get stronger, exposure to small amounts of phytonutrients is a hormetic stressor that activates several different pathways in the body, ultimately serving to reduce inflammation, enhance immunity, improve cellular communication, repair DNA damage, and even detoxify potential carcinogens. (14, 15)
It Might Affect Hormones, Fertility, and Thyroid Function
We have zero long-term data about how an all-meat diet impacts hormones, thyroid function, and fertility. I have written before about why carbohydrates are particularly important for female fertility and why very-low-carb diets may not be the best choice during pregnancy.
Carbohydrates are particularly important for supporting thyroid function since insulin stimulates the conversion of inactive thyroid hormone T4 to active T3. In fact, traditional cultures that ate largely animal products and had little access to plant foods often went to great lengths to support fertility, including eating the thyroid glands of the animals they hunted. (16)
My guess is that most modern “carnivores” are not consuming the thyroid glands of animals and are therefore at risk for suboptimal thyroid function and (at least temporary) infertility.
It Could Overtax Your Liver (If You’re Eating Lean Meat)
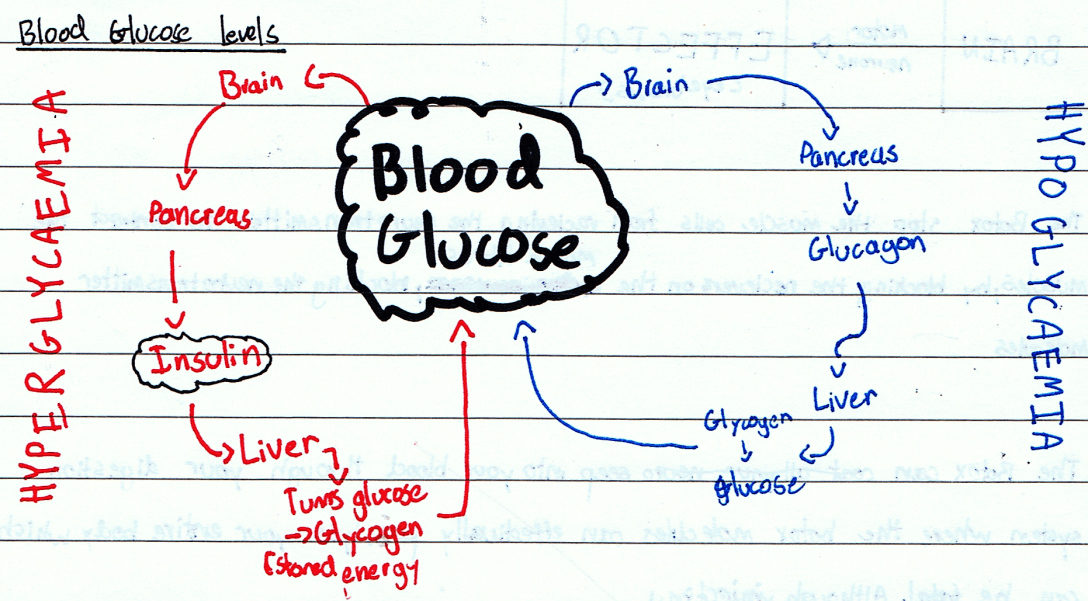
When you don’t eat sufficient carbohydrates and fat, your liver can make glucose from protein via a process called gluconeogenesis. This process creates nitrogen waste, which must be converted to urea and disposed of through the kidneys.
While this is a normal process that occurs in every human being, there is a limit to how much protein the liver can cope with safely. More than 35 to 40 percent of total calories as protein can overwhelm the urea cycle, leading to nausea, diarrhea, wasting, and, potentially, death. For pregnant women, this threshold may be as low as 25 percent of total calories. (17)
Interestingly, anthropological evidence suggests that hunters throughout history avoided consuming excess protein, even discarding animals low in fat when food was scarce. (18)
In short: When eating meat, it’s important to have a good amount of healthy fats or quality carbohydrates as well.
Is the Carnivore Diet the Ideal Human Diet?
In the last section, I outlined several potential concerns with the carnivore diet. But this leads me to another important question: even if the carnivore diet is safe, is it really the best diet for optimal health?
While you might be able to get away with a vegetarian or carnivorous diet for a short while, the evidence suggests that the ideal diet includes both animal and plant foods. Dr. Sarah Ballantyne broke this down in part three of her series “The Diet We’re Meant to Eat: How Much Meat versus Veggies.”
While you can theoretically get all of your nutrients from one group alone (and potentially supplement with any missing nutrients from the other group), we need both sets of nutrients to be optimally healthy, and consuming animal and plant foods in their whole form is the best way to accomplish this.
Five Alternatives to the Carnivore Diet
Here are some options that might provide the same therapeutic benefits that the carnivore diet can offer—but without as much potential risk.
1. A Low-Carb Paleo Diet
Some people trying a carnivore diet are going straight from the Standard American Diet to pure carnivore. Oftentimes, a low-carbohydrate Paleo template might provide some of the same benefits, including weight loss, improved insulin sensitivity, and an alleviation in autoimmune symptoms. (19, 20, 21)
2. A Fasting Mimicking Diet
A fasting mimicking diet can reverse type 1 and type 2 diabetes, alleviate age-dependent impairments in cognitive performance, and protect against cancer and aging in mice. (22, 23, 24) In humans, the fasting mimicking diet was found to significantly reduce body weight, improve cardiovascular risk markers, lower inflammation, and potentially improve symptoms of multiple sclerosis. (25, 26)
3. Periodic Prolonged Fasting
Undergoing a 72-hour fasting once every few months could also achieve many of the benefits boasted by the carnivore diet. Prolonged fasting causes organs to shrink and then be rejuvenated as damaged cells are cleared out and stem cell pathways are activated. (27)
4. A Ketogenic Diet
The ketogenic diet has been very well studied and has documented benefits for epilepsy, neurodegenerative disease, and autoimmune disease. Ketones themselves are potent anti-inflammatories. (28, 29)
5. Addressing Gut Pathologies
If a healthy lifestyle coupled with the dietary approaches above is insufficient to control your symptoms, consider working with a Functional Medicine practitioner who is knowledgeable about gut health. If you’re thinking about becoming a strict carnivore because you’re experiencing adverse reactions to even very small amounts of plant foods, that’s likely a sign of an underlying gut infection that should be addressed.
Share this with friends and family who might be considering an all-meat diet, and be sure to leave your thoughts in the comments below.
Share this post