The best diet for optimal blood sugar control & health
Author: kaitiscotland
I am a Scottish doctor who is working to improve the outcomes for people who have diabetes using a low carb diet, and advanced insulin techniques when necessary. Professionally I provide expert witness reports in the clinical forensic and family medicine areas and I also provide complementary therapies. I enjoy cooking, cinema, reading, travel and cats.
Emma and I wish you all a great Christmas in 2021.
This year has not felt as tough as 2020, mainly because we have got enough toilet paper and soap and we have almost all been doubly or triply vaccinated. We have got used to sitting at home or being in our gardens, if we are fortunate to have them, and have got used to masking up and gelling our hands.
Most of us will still have experienced some hardship and loss though. It is particularly difficult for either those who are crowded in together when they would rather not be, or being alone for very prolonged periods if you would rather not be. The stress of these things tend to be magnified over the holiday season, so particularly wish everyone in these situations a calm, peaceful and comforting Christmas.
I have been fortunate to finally retire from both GP and Police work and for the very first time in twenty years will be at home on Christmas day instead of working. I did this to allow my colleagues the day off and also to ensure that my husband made the Christmas dinner. My usual contribution is the dessert which tends to be an almond based Tiramisu, which I will make again this year.
I’m recently back from the Mayan Riviera in Mexico where my eldest son and I greatly enjoyed our first holiday together in 2 years.
This is my husband’s last year at work and he becomes a happy retiree officially on the 1st January.
I have booked off quite a lot of weeks away in 2022 and I hope we get to enjoy them. Our younger son David moved back home to work remotely soon after lockdown started so he will be here to look after our four cats when we do get away.
We are getting demented later in life than we used to! Good news?
An analysis of seven population based cohort studies in the USA and Europe found that over the last 25 years the incidence of dementia has fallen by 13% per calendar decade. The reduction tended to be greater in men compared to women.
In a large longitudinal study, moderate alcohol consumption seemed to have a beneficial effect. The Health and Retirement Study followed 20,000 middle aged and older people for nine years. When compared to those who never drank alcohol, participants who drank low to moderate quantities had higher scores for mental status, word recall and vocabulary, and lower rates of decline in all of these domains.
Although aspirin has proven benefit in the secondary prevention of cardiovascular disease, they have not been shown to reduce the incidence of dementia or cognitive decline.
20,000 older people were randomised to have either 100mg aspirin a day or placebo. Around 600 developed dementia over the five years of follow up. There was no difference between the treatment group and the placebo group however.
My comment: Although GPs and hospital doctors have been treating diabetes, hypertension and cardiovascular risk factors very aggressively over the last few decades, it is rare to get conclusive feedback that we have actually been achieving useful end points such as this, so I was delighted to see this report.
Amlodipine is one of the most commonly used calcium channel blockers in the UK. It and other drugs in this class such as Lercanipide, Diltiazem, and Verapamil, are used mainly to reduce blood pressure.
The main side effect of this class of drug is ankle swelling due to fluid retention. They can also cause gum hyperplasia, which is a swelling of the gums in the mouth so that teeth look as if they are embedded in a sponge.
The number of cases can be as high as 20% of patients. Cases tend to be under reported by dentists and under recognised by doctors.
As calcium channel blockers are the sixth most commonly prescribed drug in the UK, it is something to be aware of.
It is best treated by changing the drug and dental treatment.
Adapted from letter in BMJ by Francis Hughes, Emeritus professor of periodontology, London. 26th June 21.
Does Age at Diagnosis in Familial Diabetes Affect Type 2 Risk?
Mar 27, 2021 Editor: David L. Joffe, BSPharm, CDE, FACA Author: Mit Suthar, PharmD. Candidate, LECOM School of Pharmacy
Study of the Danish national register suggests that family members’ age at onset of diabetes could be an essential factor that is overlooked in determining type 2 risk.
A family history of diabetes is a risk factor that is widely used in screening and predicting which patients are at increased risk of developing diabetes. Family history is a practical and conveniently identifiable risk factor that provides insight into the genetic and social/behavioral contributing factors of diabetes. The familial risk depends on the number of family members affected with diabetes and the type of family relationship. However, the strongest determinants of developing type 2 diabetes are the social and behavioral elements: “obesity, physical inactivity, diet, and low socioeconomic status.”
There has been progress in understanding the connection between the etiology of type 2 diabetes and family history. Still, there is a lack of information about the effect of family members’ age at diabetes diagnosis and its relation to a patient’s risk of diabetes and their likely age of onset. The study hypothesized that “in addition to the type of family relationship and the number of family members affected with diabetes, their age at diagnosis would be associated with overall familial diabetes risk.” In a nutshell, they were trying to ascertain the effect that family members’ age at diabetes diagnosis had on an individual’s risk of developing diabetes and developing diabetes. This hypothesis was studied by using a national register that covered the total Danish population.
A national register-based open cohort study of patients living in Denmark between 1995 and 2012 was performed. The study population consisted of individuals 30 years old or older without a diabetes diagnosis but who had access to their parent’s identity and information. The open cohort design allowed the addition of patients who turned 30 years old during the observation period. These specific criteria meant that most individuals included in the study were born between 1960 and 1982. This population was followed from January 1, 1995 (or the date of cohort entry) until they emigrated, or death, or until December 31, 2012.
After the inclusion and exclusion criteria were implemented, the study population comprised 2,000,552 individuals in 1,107,915 families, with the median age at entry into the study being 30 years old. These individuals were followed for a median of 14 years, and 76,633 new cases of type 2 diabetes were observed. They found that men and women had similar sociodemographic backgrounds and familial diabetes indicators. Still, a more significant proportion of women (42%) had completed more than 15 years of education than men (31%).
Furthermore, and more importantly, they found that: “Compared with individuals of the same age and sex who did not have a parent or full sibling with diabetes, the highest risk of developing type 2 diabetes was observed in individuals with family members diagnosed at an early age.“ The IRR was also increasingly lower when family members had diabetes diagnosed at a later age. “3.9 vs. 1.4 for those with a parental age at diagnosis of 50 or 80 years, respectively; and 3.3 vs. 2.0 for those with a full sibling‘s age at diagnosis of 30 or 60 years, respectively.“
The data collected from the national registers of Denmark illuminated how different combinations of exposure to familial diabetes can increase an individual’s risk of developing type 2 diabetes. The researchers found that individuals with a family member who was diagnosed with diabetes at an earlier age are more likely to develop diabetes and unfortunately also develop it at an earlier age, compared to individuals with family members who developed diabetes at a later age.
These findings are significant as they highlight the importance of understanding the complex interactions between “genetic diabetes determinants and the social, behavioral and environmental diabetes determinants,” which follow families across generations. There is a strong argument for the inclusion of recording an age of onset of diabetes for those family members we include in the family history when trying to screen for and predict the risk of developing type 2 diabetes in patients. The relative ease with which such data can be obtained and the highly relevant nature of the findings can significantly improve individuals’ identification, especially those at a higher risk of developing diabetes at a younger age vs. those who are more likely to develop diabetes later in life. This information can benefit many family members and not just the patient who is being screened.
Practice Pearls:
Family history is a vital independent risk factor for developing type 2 diabetes. Right now, the familial risk depends on the number of family members affected by the disease and the nature of the family relationship, but the age of onset of diabetes could be an essential factor that is overlooked.
The nationwide open cohort found that patients with a family member who was diagnosed with diabetes earlier in life are more likely to develop diabetes, and also at an earlier age, than those patients whose family members developed diabetes at a later age.
The benefits of obtaining the age of diagnosis of family members mean that it should become part of recording the diabetes family history. These individuals with family members who developed diagnosis at an earlier age could benefit from a more detailed risk factor assessment as well as individualized prevention strategies.
Schwarz, et al. “Effect of Familial Diabetes Status and Age at Diagnosis on Type 2 Diabetes Risk: a Nationwide Register-Based Study from Denmark.“Diabetologia, 19 Feb. 2020, link.springer.com/article/10.1007/s00125-020-05113-8.
Mit Suthar, PharmD. Candidate, LECOM School of Pharmacy
My comment: Although it seems common sense that the younger age at diagnosis and the number of relatives affected with type 2 diabetes, the higher a persons individual risk seems, this is the study that nails it.
Flour (omit if gluten intolerant or on low carb diet)
Beef broth
2 cups full-bodied dry red wine
1/4 cup unsalted butter
Salt and pepper
Directions
Flour the beef, or perhaps not, and brown the pieces in the butter, taking them out of the pot with a slotted spoon and setting them aside when brown.
Slice the onions into rounds and brown them in the same pot, add a ladle of broth and simmer until the broth has evaporated. Add the meat, the spices, the bay leaf, salt and add a pinch of sugar. Then add the wine, bring it all to a boil, reduce the heat to a slow simmer and cook, covered, adding more broth as necessary to the meat submerged.
After about 2 hours or when the meat is tender, add a grinding of pepper and serve.
Type 2 Diabetes Delayed by Menopause Hormone Therapy
Mar 16, 2021 Editor: David L. Joffe, BSPharm, CDE, FACA Author: Mit Suthar, PharmD. Candidate, LECOM School of Pharmacy
The mechanisms by which estrogens / hormone therapy improve glucose homeostasis and delay diabetes are not completely understood.
Franck Mauvais-Jarvis, MD., director of the Tulane Diabetes Research Program at Tulane University Health Sciences Center, New Orleans, explained at the Annual World Congress on Insulin Resistance, Diabetes & Cardiovascular Disease: “During the menopause transition, women accumulate metabolic disturbances, including visceral obesity, systemic inflammation, insulin resistance, dyslipidemia, and hypertension. They also lose muscle mass. Some of these abnormalities are partially explained by chronological aging, but they are also caused by estrogen deficiency. There’s a synergism between aging and estrogen deficiency.”
Almost 30 years ago, researchers investigated the connection between postmenopausal hormone use and the subsequent incidence of non-insulin dependent diabetes in a prospective cohort of 21,028 postmenopausal US women aged 30-55 years. These women were registered in the Nurse’s Health Study and monitored for 12 years (Ann Epidemiol. 1992;2[5]:665-73).
Interestingly, during this study they found that the patients who were on hormone therapy experienced a 20% reduction in the incidence of type 2 diabetes. A newer study from 2009 analyzed the association between the use of hormone therapy and new-onset diabetes in 63,624 postmenopausal women. These patients were enrolled in the prospective French cohort of the Etude Epidemiologique de Femmes de la Mutuelle Générale de l’Education Nationale (E3N) and followed for 15 years (Diabetologia. 2009;52[10]:2092-100). This study also found that participants who were taking hormone therapy also experienced a 20% reduction in the incidence of type 2 diabetes.
In another study called the Heart and Estrogen/Progestin Replacement Study researchers evaluated the effect of hormone therapy on fasting glucose level and incident diabetes. 20 US centers reported on 2,763 postmenopausal women with coronary heart disease (Ann Intern Med. 2003;138[1]:1-9). The study participants received 0.625mg of conjugated estrogen with 2.5mg of medroxyprogesterone, or placebo, and were followed for 4 years. The research discovered that patients who were treated with hormone therapy had a 35% reduction in the incidence of diabetes.
Dr. Mauvais-Jarvis stated that the strongest data came from the Women’s Health Initiative (WHI), which was a randomized, double-blind trial (Diabetologia. 2004; 47[7]:1175-87). This trial compared the effect of daily 0.625mg conjugated estrogen and 2.5mg medroxyprogesterone acetate with placebo during 5.6 years of monitoring. This trial also revealed a 20% decrease in the incidence of diabetes after 5 years. The researchers found that the protection from diabetes was present whether the WHI participants took just estrogen alone or estrogen plus medroxyprogesterone (N Engl J Med. 2016;374:803-6).
Results from research published in 2006 from a meta-analysis of 107 trials (Diabetes Obes Metab. 2006;8[5]:538-54) found that in women without diabetes, hormone therapy decreased the HOMA-IR (Homeostatic Model Assessment for Insulin Resistance) score by 13% and incidence of type 2 diabetes by 30%. Women with diabetes who took hormone therapy had their fasting glucose reduced by 11% and HOMA-IR by 36%.
Dr. Mauvais-Jarvis explains that the mechanisms by which estrogens improve glucose homeostasis are not completely understood. “One of the most important [mechanisms] is a decrease in abdominal fat, which improves insulin resistance and systemic inflammation. However, in the WHI, it was clear that the improvement in HOMA-IR was independent from the body weight and fat. Estrogen has also been found to increase insulin clearance and sensitivity, increase glucose disposal and effectiveness and decrease sarcopenia. There are fewer than 20 studies looking at beta-cell function. Half of them have shown that estrogen improves insulin secretion.” The idea that the benefits of hormone therapy are independent of weight loss for reducing the incidence of diabetes is certainly encouraging.
Significant factors about the benefits and disadvantages of hormone therapy include the route of administration, and adverse effects of the therapies. Oral estrogens can increase liver exposure to estrogen, increase triglycerides, and increase clotting factors, but an advantage is that oral estrogen is a cheaper form than the transdermal form. Transdermal delivery of estrogen does not raise triglycerides, clotting factors, or inflammatory factors, and presents less exposure to the liver.
Dr. Mauvis-Jarvis and colleagues also evaluated the effect of conjugated estrogens plus bazedoxifene in mice (Mol Metab. 2014;3[2]:177-90). The reason bazedoxifene was combined to estrogen was to preserve the beneficial effects of estrogen but block the estrogen in the breast and uterus, thus decreasing the risk of cancer.
The unforeseen benefits of menopausal hormone therapy cannot be ignored in regard to the decreased incidence of diabetes in patients who take these hormonal therapies. While it is doubtful that hormone therapy will ever be approved for a diabetic indication due to the various complexities of said therapy, hormonal therapy should not be denied to patients with an approved indication who are at increased risk for developing diabetes.
Practice Pearls:
Menopausal hormone therapy can significantly reduce the incidence of diabetes in patients who have an indication for hormone therapy and are at risk for developing diabetes.
Both older and more recent trials have demonstrated this reduction in incidence, which is around 20%
The mechanisms by which estrogens improve glucose homeostasis are not completely understood and the risks of estrogen therapy, such as cancer risk, must be accounted for on a patient by patient basis
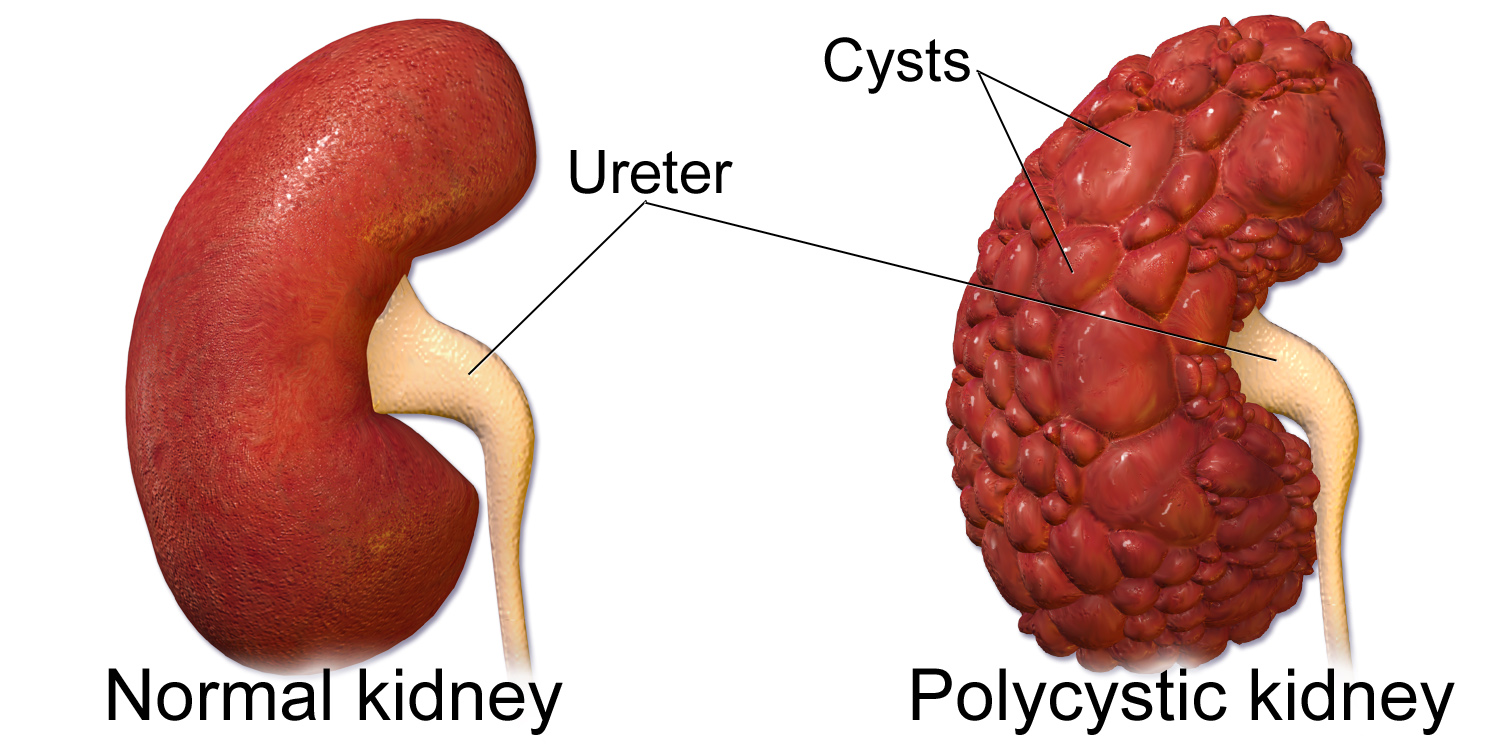
Teresa Rodriguez is a Florida USA specialist dietician who has undertaken training with the Charlie Foundation to provide help to patients who have severe kidney disease of various types. Some conditions, previously thought to be untreatable, such as Polycystic Kidney Disease respond to the ketogenic diet and the quality of life and life expectancy for these people has been transformed.
Teresa sees patients in person and coaches them online and via Facebook. She is expecting her book, aimed at both physicians and patients, Keto for Kidney Disease, to be published in March 22.
Teresa comes from Puerto Rico and speaks fluent Spanish and American English and can provide learning in both languages.
I was one of several doctors who were treated to an online presentation by Teresa recently, and was amazed to see how different her approach and results are compared to NHS “usual” treatment and results.
I was taught that there wasn’t really much you could do about Polycystic Kidneys except for dialysis and transplantation when the kidneys eventually failed. She explained that PKD is actually a metabolic condition and that it responds to a ketogenic diet of usually 20g carbohydrate a day. There can be other aggravating factors such as oxalate overload and the kidney needs support to avoid the formation of kidney stones. Many patients will need to drink lemon juice in the mornings and have a much higher fluid intake than usual.
She optimises the patient’s diet based on the results of a detailed clinical history and blood and urine results. She finds that Cystatin C is a much more reliable predicator of kidney function than standard tests such as Creatinine Clearance. She often has to modify drug prescriptions. The blood pressure must be kept within normal limits to reduce deterioration in kidney function but Calcium channel blockers are not beneficial in PKD compared to ACE inhibitors and Sartans. Metformin, however is beneficial.
There is increasing interest in Ketogenic Diet Therapy and Therapeutic Carbohydrate Restriction worldwide.
Metformin use was associated with lower inflammatory markers before surgery, leading to improved outcomes post-surgery.
Around a third of patients >65 years in the U.S. have type 2 diabetes (T2DM). Due to diabetes complications, renal and cardiac comorbidities are common in many patients, leading to impaired inflammatory responses and reduced time to recovery. Also, around half of this patient population undergoes surgical treatment during their lifetime. Therefore, these effects may lead to increased morbidity and mortality post-surgery.
Patients with T2DM have commonly been prescribed metformin as first-line therapy. In addition to its impact on blood glucose control, it has been shown to reduce chronic inflammation. These effects have been studied in diseases linked with the aging process, such as cardiovascular and renal diseases. Previous literature regarding the use of metformin has shown that it reduces all-cause mortality and cardiovascular and renal complications. However, whether metformin use pre-surgery can improve patients’ outcomes post-surgery was not studied before.
A new study aimed to assess the effect of metformin on post-surgical outcomes in patients with T2DM. The study design was retrospective, including patients with T2DM who underwent surgery and were eligible for metformin use. It excluded patients with type 1 diabetes or impaired renal function, since metformin is not indicated in those cases. The investigators compared the patients’ outcomes based on whether they received metformin before surgery or not. Since metformin’s effect on inflammation is based on its use over time, patients’ glycemic control was not considered in the enrollment process. They included patients with an increased risk of mortality or readmission.
The study data was collected from January 2010 to January 2016, and the follow-up continued to December 2018.
Metformin exposure was considered if the patient received at least one prescription within six months before surgery and prescribed the last doctor’s prescription before surgery. Patients who did not meet these criteria were considered not exposed to metformin and fell in the comparison group. Those who are not indicated to use metformin were excluded from the study. The study identified the primary outcome to be 90 days mortality post-surgery. Additionally, secondary outcomes were identified, including 30-day mortality, readmission within three months post-surgery, 5-year survival rate, and the level of the inflammatory marker neutrophil to leukocyte ratio (NLR) pre-surgery.
The study included 5,460 patients who were matched at a 1:1 ratio between the study groups. Patient characteristics were similar between the groups. In the metformin group, around 2% of deaths were reported within a month of surgery. Also, 3% of deaths were reported after three months and 13% in the 5th year. On the other hand, the non-metformin group showed a similar 2% death rate in the first month, but the rates increased to 5% and 17% by three months and five years, respectively. The risk reduction associated with metformin use is considered statistically significant (1.28%; 95% CI, 0.26–2.31). The results also indicate that metformin use was associated with a statically significant reduction in 90-day and 5-year mortality. These outcomes were similar to most surgical interventions except in neurosurgery, which did not show a significant risk reduction with the use of metformin. When comparing hospital readmissions, metformin use was associated with significantly lower readmission rates from 1 to 3 months after discharge than patients who did not receive metformin. Moreover, patients in the metformin group had lower NLR levels before surgery.
The study findings suggest that metformin has additional mechanisms of action to its known means for glycemic control. The reduction of the NLR before surgery is associated with a decrease in morbidity and mortality post-surgery. The study has several limitations, one of which the possibility of confounding variables due to its design. One reason is that the type of surgery was evenly distributed between cohorts. Different surgeries can cause additional surgical stress to the patients, which may affect the study’s outcome. Also, the retrospective nature may introduce selection bias during the data collection phase. Furthermore, the author indicated that the mortality and admission rate might have been misrepresented.
Practice Pearls:
Metformin use in patients with T2DM is associated with a reduced mortality risk post-surgery.
Readmission post-discharge is reduced with metformin use before surgery in patients with T2DM.
Patients with T2DM on metformin have lower inflammatory markers before surgery, leading to improved outcomes post-surgery.
Reitz, Katherine M. et al. “Association Between Preoperative Metformin Exposure And Postoperative Outcomes In Adults With Type 2 Diabetes”. JAMA Surgery, vol 155, no. 6, 2020, p. e200416. American Medical Association (AMA), doi:10.1001/jamasurg.2020.0416.
Campbell, Jared M. et al. “Metformin Reduces All-Cause Mortality And Diseases Of Ageing Independent Of Its Effect On Diabetes Control: A Systematic Review And Meta-Analysis.” Ageing Research Reviews, vol 40, 2017, pp. 31-44. Elsevier BV, doi:10.1016/j.arr.2017.08.003.
Abdullah Al-Ajmi, PharmD Candidate, Skaggs School of Pharmacy and Pharmaceutical Sciences
If you think these are the healthy option, you must read this post
Industrial seed oils are sold in big plastic containers of bright gold liquid, and although some of us will buy these to deep and shallow fry foods at home, most of the seed oils we eat will be hidden in processed foods, often marketed as convenient and healthy.
When ingested, these oils cause a low grade inflammatory process that can aggravate and sometimes cause such diverse conditions as: diabetes, obesity, cardiovascular disease, macular degeneration of the eyes, osteoarthritis, gut pain, asthma, autoimmune illnesses, dementia and mental health problems.
Kriss Kresser explains why these oils should be avoided and what fats to eat instead. Of course, this largely means ditching processed foods, if you haven’t already.
What do the new ADA guidelines for HbA1C have to say about treating children and adolescents with type 1 diabetes?
Recently, the American Diabetes Association (ADA) recommended lowering the target hemoglobin A1C (HbA1C) guidelines for children with type 1 diabetes (T1D).
A study conducted by Redondo et al. has shown that stricter controls of HbA1C within this population resulted in improved patient outcomes. Specifically, it was revealed that chronically elevated blood glucose levels in children could lead to increased rates of several serious effects, such as abnormal brain development; cardiac issues including stroke, coronary, peripheral heart disease; and other diabetic complications, nephropathy, neuropathy, and retinopathy. Better control of blood glucose levels lowered these events’ incidence and improved mortality rates in children and adolescents with T1D. http://imasdk.googleapis.com/js/core/bridge3.476.0_en.html#goog_25686799Volume 0%
Regarding abnormal brain development, one meta-analysis (n=1619) showed that patients with T1D had lower inhibition, working memory, and executive function compared to control subjects. In a study regarding microvascular diseases, patients with lower HbA1C had a significantly lower risk of microvascular diseases than patients with higher HbA1C (mean Hba1C 8.06% vs. 9.76%). A study conducted by the Swedish National Diabetes Register found a risk over fourfold for all-cause mortality, over sevenfold for cardiovascular mortality, and elevenfold for cardiovascular disease in patients diagnosed with T1D under age ten compared to the control group.
Due to this study’s results, the ADA 2020 Standards of Medical Care recommends that children and adolescents with T1D target an HbA1C goal of less than 7%. This is a change from their 2019 guidelines, which had a target HbA1C goal of less than 7.5%.
The study suggests that more intensive insulin therapy is the preferred strategy to treat children and adolescents with T1D. Instead of simply treating a patient’s hyperglycemia with insulin, it would be more beneficial to more aggressively bring blood glucose levels to a normal range. More aggressive blood glucose treatment seems to be the best strategy that results in a lower incidence of diabetes-related complications and long-term organ damage.
However, caution should be used in this approach as more aggressive insulin therapy and lower HbA1C targets often result in a higher incidence of hypoglycemia. Symptoms of hypoglycemia are severe and can include dizziness, seizures, coma, and death. Despite this, the study has found that the incidence of hypoglycemia in children and adolescents with T1D has been steadily declining over the past three decades. The Danish Adult Diabetes Database (DADD) found an annual decrease of 8.4% in hypoglycemia incidence in children under 15 with type 1 diabetes from 1995-2016. Another similar study showed no significant difference in hypoglycemia rates in children who had an A1C <7% compared to children who had an A1C between 8-9% (n=1,770). Over this time, the lowered hypoglycemia rates coincide with innovations in drug therapies and technologies, such as insulin analogs, insulin pumps, and continuous glucose monitoring.
These innovative technologies make it easier than ever to keep a patient’s HbA1C within a prespecified range and reduce the risk of hypoglycemia. The ADA still recommends a target of 7.5% for patients too young to properly articulate hypoglycemic symptoms, or patients who do not have access to these innovative technologies. An HbA1C score of less than 8% is acceptable for patients with a severe history of hypoglycemia or a shortened life expectancy due to other pre-existing conditions.
Practice Pearls:
The ADA recently recommended lowering the target HbA1C from 7.5% to 7% for children with type 1 diabetes.
Lowering the target HbA1C in children and adolescents with type 1 diabetes reduces the risks of developing diabetic complications such as nephropathy, neuropathy, and retinopathy, abnormal brain development, and cardiac disorders, and improves mortality.
Although more aggressive insulin regimens can result in hypoglycemia, hypoglycemia rates in children and adolescents with type 1 diabetes have decreased over the past three decades due to innovative new technologies and therapies such as insulin analogs, insulin pumps, and continuous glucose monitoring.