The best diet for optimal blood sugar control & health
Author: kaitiscotland
I am a Scottish doctor who is working to improve the outcomes for people who have diabetes using a low carb diet, and advanced insulin techniques when necessary. Professionally I provide expert witness reports in the clinical forensic and family medicine areas and I also provide complementary therapies. I enjoy cooking, cinema, reading, travel and cats.
Adapted from BMJ 4 May 2024 Weights, resistance bands, and rest days are best for tendinopathy.
A systemic review and meta-analysis by Pavlova and Shim, published in the Journal of Sports Medicine 2023, indicates that planned exercise using weights or resistance bands with rest intervals gives better results than exercising every day, particularly with body weight exercises.
People with diabetes are considerably more prone to tendinopathy than the general population, so these findings may be helpful to them.
Tendinopathy is diagnosed when tendons become painful, stiff or swollen. It can affect both adults and children and tends to occur in the Achilles tendon at the heel, shoulder, elbow, knee and hip.
Although exercise is recommended it hasn’t been clear what specific exercises help the condition and what the training pattern should be to maximise effectiveness. Improving disability, function, pain, movement and quality of life are important for people who suffer from these conditions.
This study included 110 studies covering 4,000 people from Europe, Australia and the USA. Most of the exercise regimens had been prescribed or delivered by physiotherapists.
The study found that people improved more if they used dumbells, loaded backpacks or resistance bands rather than bodyweight only in resistance exercises. Also, rest days between sessions gave better results than daily exercises. The results were the same no matter the tendon damage site.
The authors suggest that at least one day of rest between the exercise sessions is necessary to maximise improvement. The number of repetitions and sets necessary did not become clear after the analysis.
My comment: So many people suffer from musculo-skeletal pain and research like this is very helpful. I’m a daily exerciser and I found that my chronic back pain got better by having more than one day between intense resistance workouts. Previously it had been alternate day resistance exercise alternating with either aerobic exercise or yoga/stretching. So many of us have the idea that more is better when really we would be better off doing less. Weights and resistance bands give more flexibility regarding the force exerted on the muscle and tendon so may lend themselves to progressive overload than body weight exercise.
Adapted from Statins: the risks and statistics by George Winter, Freelance writer and Fellow of the Institute of Biomedical Science. British Journal of Nursing 2023 Vol 32 No 20.
In a randomised trial of 3000 participants, Carling et al in 2009 concluded that when presented with the benefits of taking statins as a relative risk reduction, participants were more likely to accept treatment compared to when the absolute risk was given.
In a meta-analysis of 21 randomised controlled trials, Byrne et al in 2022 found reductions in AR of 0.8% for all cause mortality, 1.3% for myocardial infarction, 0.4% for stroke in those randomised for treatments with statins compared with control. The RR reduction for these were 9%, 29% and 14% respectively.
Diamond and Leaverton in 2023 consider that undue emphasis on RR reduction compared to AR reduction has led healthcare providers and the public to overestimate concerns about high cholesterol and to be misled as to the magnitude of the benefits of cholesterol lowering therapy.
Diamond and Leaverton re-evaluated the JUPITER trial of rosuvastatin. There were 18 thousand participants and there was a reported RR of 54% for fatal myocardial infarction. In absolute terms, the incidence of fatal MIs was 0.76% in the control group and 0.35% in the rosuvastatin treated group.
It would seem reasonable and good practice for both RR and AR to be discussed with patients when it comes to initiating treatments such as statins.
Why exercise is one of the best tools we have for cancer prevention.
Let’s start with the simple fact that a lot of cancer diagnoses are simply down to ‘bad luck’.
You can do everything right and still get cancer.
This is a somewhat depressing fact, given its leading position as a cause of death.
The other leading cause of death, cardiovascular disease, is mostly preventable.
Cancer – Less so.
But that does not mean you cannot tilt the odds in your favour.
And regular exercise, it seems, might be a good way of doing so.
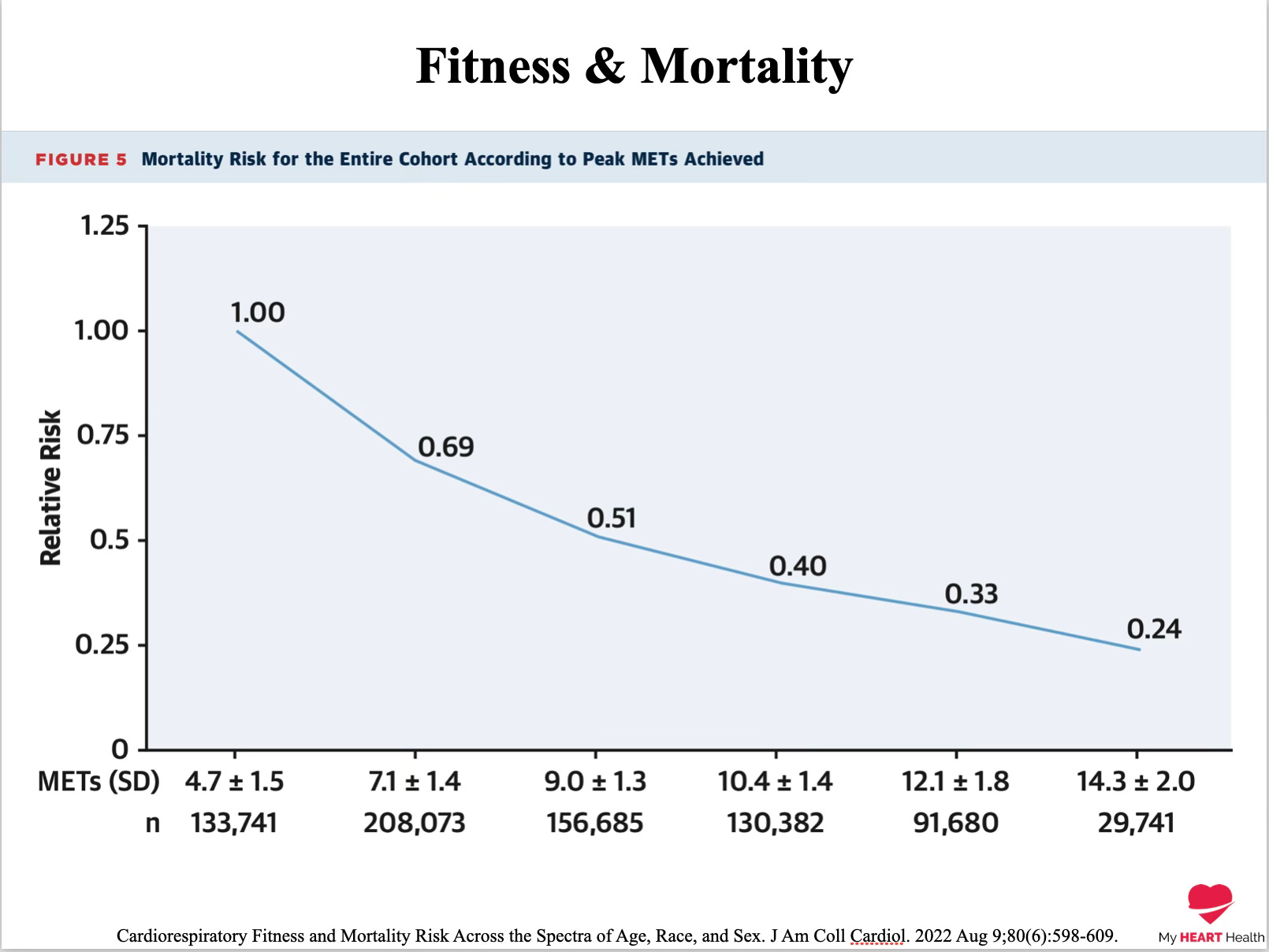
Regular exercise and high levels of physical fitness have been consistently associated with longer lifespans and a substantially reduced risk of dying from any cause¹.
If exercise reduces all-cause mortality, it seems safe to say that it is reducing cardiovascular and cancer deaths.
Over a 10-year period, those in the highest fitness levels had an 11% reduction in the risk of cancer².
But this 11% figure masks the fact that not all cancers are impacted equally.
Exercise has little effect on some cancers, while it has a much bigger effect on others.
While the risk of gastric/stomach cancer is reduced by only about 5%, the reductions in other cancer types are even greater.
Breast Cancer – 13% Reduction
Oesophageal Cancer – 18% Reduction
Liver Cancer – 18% Reduction
Lung Cancer – 25% Reduction
Colorectal Cancer – 26% Reduction
The impact of exercise on cancer even extends beyond the original diagnosis and has been shown to reduce the likelihood of recurrence of cancer³.
Regular exercise in those who have already been diagnosed with cancer has been associated with:
A reduced chance of dying from a breast cancer diagnosis by 40% compared to those with breast cancer who did not exercise regularly⁴.
A reduced risk of death from colorectal cancer by 30%⁵.
The question is WHY exercise might be associated with such benefits with respect to cancer.
Regular exercise and high fitness levels are associated with lower rates of obesity.
Obesity is the second leading cause of preventable cancers after smoking⁶.
Please reread that line again.
It should hit you like a ton of bricks. If it doesn’t, you are not getting the magnitude of the problem that is preventable.
The likely driver of the cancer risk conferred by obesity is probably related to higher levels of insulin resistance and metabolic syndrome.
A diagnosis of metabolic syndrome significantly increases your risk of several leading cancers⁷:
Postmenopausal Breast Cancer – 52% Increased Risk
Hepatocellular Cancer – 81% Increased Risk
Colorectal Cancer – 30-40% Increased Risk
Pancreatic Cancer – 55% Increased Risk
But insulin resistance and metabolic syndrome are not the only drivers of risk.
Cancer As A Breakdown Of Immune Function
The hallmark of cancer is the uncontrolled replication of cells.
But the cells in your body are continually replicating.
The mechanisms of replication usually do an excellent job at producing exact copies of cells, but sometimes replication errors occur, which can lead to the development of cancer⁸.
The immune system’s job is to constantly search for these poorly replicated cells and destroy them.
In truth, we are probably creating very early cancerous cells throughout our lives, but because of our immune system, they do not get the opportunity to progress into fully formed cancers.
Natural Killer Cells are one of the key agents for targeting abnormal precancerous cells.
A properly functioning immune system then is essential for cancer protection.
Hereditary Cancers and The Role Of The Immune System
Lynch syndrome is a genetic colorectal cancer disorder where 60% of carriers go on to develop colorectal cancer over their lifetime⁹.
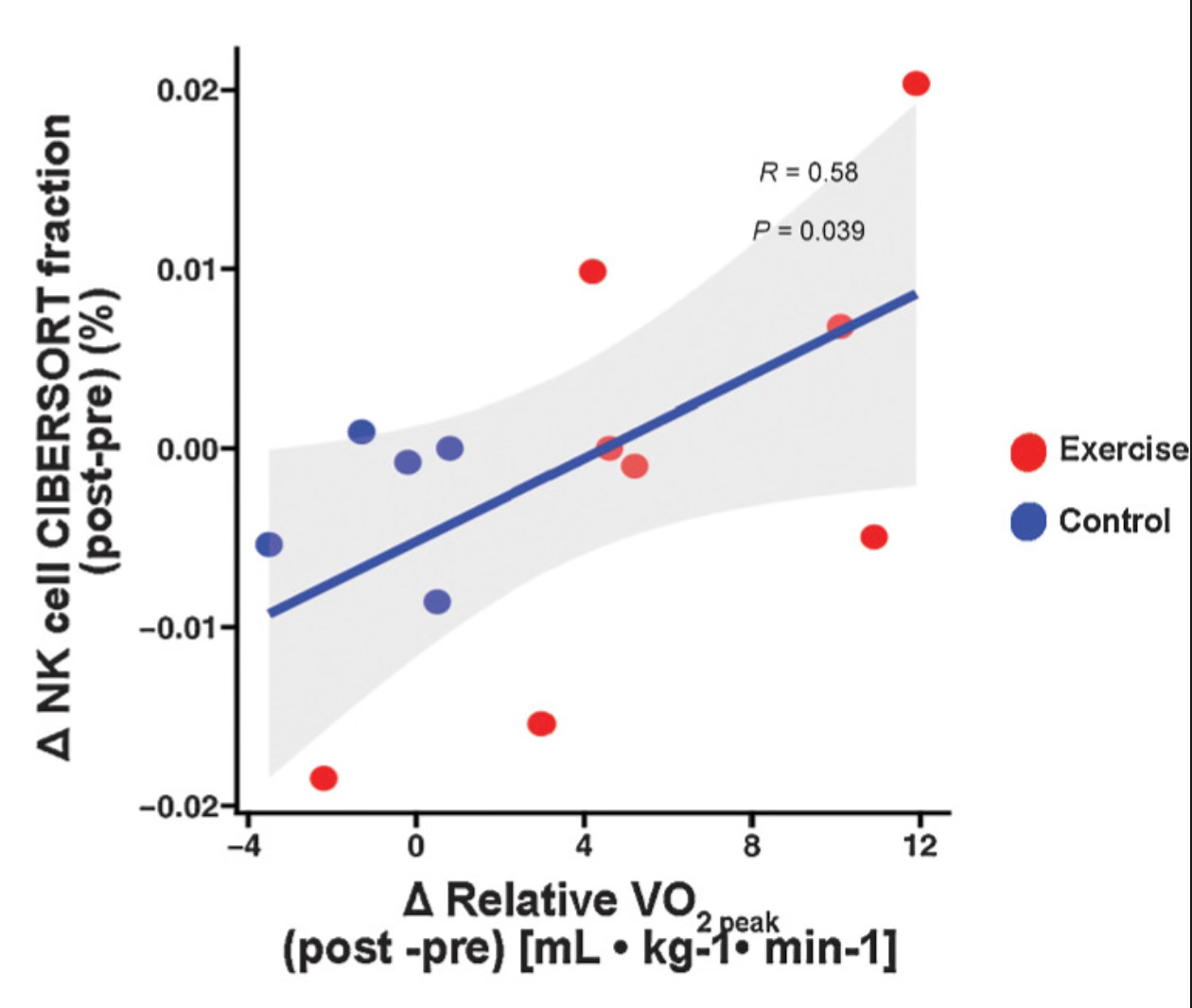
A recent study examined the question of whether regular exercise in such a high-risk group for cancer would impact the number of natural killer cells, which are important tools for destroying early cancer cells.
Those who did 45 minutes of high-intensity exercise three times per week for a year had significantly higher levels of natural killer cells¹⁰.
The higher levels of natural killer cells are likely to explain at least some of the protection regular exercise confers when it comes to cancer prevention.
Regular exercise also influences a variety of other cellular mechanisms that modulate cancer risk, including beneficial changes in¹¹:
Cell Growth Regulators – IGF1 & IGFBP3.
Suppression of RAS oncogenes.
Higher levels of proteins involved in cellular repair.
Enhanced activity of regulators of apoptosis and cellular growth.
Tilting Odds
The best way of not dying from cancer is to not get cancer.
Unfortunately, much of that risk is simply down to ‘Bad Luck’.
However, it is clear that regular exercise can play a crucial role in decreasing the odds of developing cancer, and the mechanisms by which it does so are becoming increasingly clear.
We need all the help we can get.
Keep the odds on your side.
1
Cardiorespiratory Fitness and Mortality Risk Across the Spectra of Age, Race, and Sex. J Am Coll Cardiol. 2022 Aug 9;80(6):598-609.
2
Association between physical activity and cancer risk among Chinese adults: a 10-year prospective study. Int J Behav Nutr Phys Act 19, 150 (2022).
3
Physical Activity Reduces the Risk of Recurrence and Mortality in Cancer Patients. Exerc Sport Sci Rev. 2020 Apr;48(2):67-73.
4
Physical activity in breast cancer survivors: A systematic review and meta-analysis on overall and breast cancer survival. Breast 2019; 44:144-152.
5
American College of Sports Medicine Roundtable Report on physical activity, sedentary behavior, and cancer prevention and control. Medicine and Science in Sports and Exercise 2019; 51(11):2391-2402
6
Cancer is a Preventable Disease that Requires Major Lifestyle Changes . Pharmaceutical Research, Vol. 25, No. 9, September 2008
7
Mendonça FM, et al, Metabolic syndrome and risk of cancer: Which link? Metabolism (2014),
8
Roles of the immune system in cancer: from tumor initiation to metastatic progression. Genes Dev. 2018 Oct 1;32(19-20):1267-1284.
9
Cancer risks by gene, age, and gender in 6350 carriers of pathogenic mismatch repair variants: findings from the Prospective Lynch Syndrome Database. Genet Med. 2020 Jan;22(1):15-25.
10
Exercise Training Reduces the Inflammatory Response and Promotes Intestinal Mucosa-Associated Immunity in Lynch Syndrome. Clin Cancer Res 1 November 2023; 29 (21): 4361–4372.
11
Why exercise has a crucial role in cancer prevention, risk reduction and improved outcomes, British Medical Bulletin, Volume 139, Issue 1, September 2021, Pages 100–119,
If you liked this post please consider sharing it?
As with all the material on this site it is not medical advice and is for general informational purposes only. None of the information provided constitutes the practice of medicine, or any professional healthcare services. No doctor patient relationship has been formed. Information contained on this platform is used at the readers own risk. Readers of this information should not delay or disregard in obtaining professional medical advice or treatment for any health related issue. The information presented is in no way a substitute for medical advice.
My comment: There is new research indicating that mitochondrial function greatly improves with exercise. It reduces the potential for DNA changes that can lead to cancer and in cellular degeneration. I didn’t write a specific blog about this as the scientific detail is overwhelming to me and I already keenly advocate exercise across all ages.
2 tsp. ground cinnamon 4 tsp. ground cumin 3 tsp. ground coriander 2 T. freshly grated ginger 1 T. all-purpose flour (or arrowroot) 1 ½ tsp. salt, plus more to taste ¼ tsp. freshly ground pepper, plus more to taste 2 lb. lean leg of lamb, cut into 1-inch cubes 3 T. olive oil 4 T. unsalted butter 2 large onions, thinly sliced 1 T. sugar 3 large cloves garlic, peeled and minced (about 1 ½ T.) 3 c. beef stock 1 28-oz. can whole Italian plum tomatoes 2 pieces star anise 2 cinnamon sticks, about 3 inches long 2 medium carrots, peeled and cut into ½-inch rounds 2 lb. sweet potatoes, peeled and cubed 12 oz. fresh spinach (optional) washed ½ c. dried tart cherries ½ c. dried pitted prunes, cut in half freshly grated nutmeg, for sprinkling
1. In a medium mixing bowl, combine the ground cinnamon, 2 tsp. cumin, 1 tsp. coriander, flour, ½ tsp. salt, and ¼ tsp. pepper. Toss the lamb pieces with the spice mixture to coat.
2. In a Dutch oven or a large saucepan, heat 2 T. olive oil over medium-high heat. Add the lamb in two to three batches, in a single layer, and sear until dark brown on all sides, about six minutes per batch. Add the remaining T. olive oil during searing if pan becomes dry. Remove the lamb pieces and set aside.
3. Reduce heat to medium; add I T. butter. Add onions and sugar; cook 10 minutes, stirring frequently, scraping up brown bits on bottom of pan while stirring the onion.
4. Reduce heat to medium low, add the minced garlic, and cook until brown and well caramelized, about 15 minutes.
5. Stir in the stock, tomatoes, star anise, cinnamon sticks, carrots, remaining 2 tsp. cumin, 2 tsp. coriander, the fresh ginger, remaining 1 tsp. salt, and reserved lamb. Bring to a boil, reduce heat to medium, and simmer, stirring occasionally, uncovered, for about 1 hour, until lamb is tender and sauce is thick.
6. Meanwhile, place sweet potatoes in a large saucepan; cover with cold water. Bring to a boil, reduce heat to medium, and simmer, uncovered, for 15 minutes, until very tender when pierced with a fork. Drain potatoes, and return to saucepan. Dry potatoes, over medium heat, for 1 minutes. Pass potatoes through a food mill into a medium bowl. Stir in remaining 3 T. butter; add salt to taste. Set aside, loosely covered.
7. Preheat oven to 325 degrees. If using spinach, place in a large skillet over medium-high heat. Season to taste with salt and pepper, cover, and cook until wilted, about 1 ½ minutes. Drain, and rinse under cold water to stop the cooking. Set aside. 8. Remove the star anise and cinnamon sticks from the stew. Stir in the cherries and prunes. Transfer mixture to a deep 2-qt. Casserole, and place a layer of spinach, if using, over the stew. Spoon the sweet potato mixture onto the stew. Place on a baking sheet, and bake for 30 minutes. Sprinkle with freshly grated nutmeg.
2 ½ pounds, about 12 Roma tomatoes, halved 3 medium carrots, peeled and cut into small chunks Extra virgin olive oil Salt Black pepper 2 medium onions, chopped 5 garlic cloves, minced 14 oz container of canned crushed tomatoes 1 bunch (2 ounces) fresh basil leaves 1 teaspoon dried thyme leaves 1 teaspoon dried oregano ½ teaspoon sweet paprika ½ teaspoon ground cumin 3 cups water
Directions
Preheat your oven to 450°F.
In a large mixing bowl, toss the tomatoes and carrots with a generous drizzle of extra virgin olive oil, and a pinch of salt and pepper. Transfer to a large baking sheet and spread well in one layer.
Roast in the heated oven until the tomatoes have deflated and begun to char at the edges, about 45 minutes. Set aside for a to cool. You can even do this step a day in advance.
Transfer the roasted carrots and tomatoes (along with their skin and seeds) to the bowl of a food processor fitted with a blade. Add a splash of water and blend until the vegetables have broken down and combined. Some texture is nice, so stop the processor before it becomes a super smooth puree.
In a large pot, heat 2 tablespoons of extra virgin olive oil over medium-high heat. When the oil begins to shimmer, add the onions and cook, stirring, until softened, about 3 minutes. Add the garlic and cook briefly until golden, about 1 minute.
Pour the roasted tomato mixture into the pot with the onions. Stir in the crushed tomatoes, basil, thyme, oregano, paprika, cumin, and 3 cups of water. Season with salt and pepper. Bring to a boil, then lower the heat and cover, leaving the lid slightly ajar to allow some steam to escape. Let simmer for about 60 minutes.
Check the consistency of the soup. If you would prefer a smoother texture then use a stick blender to puree the mixture further.
Adapted from Alzheimer’s and Dementia 15(2019) 625-634
A ketogenic drink improves brain energy and some measures of cognition in mild cognitive impairment
Melanie Fortiera, *, Christian-Alexandre Castellanoa et al.
Research Center on Aging, CIUSSS de l’Estrie – CHUS, Sherbrooke, Quebec, Canada.
Abstract Introduction:
Unlike for glucose, uptake of the brain’s main alternative fuel, ketones, remains normal in mild cognitive impairment (MCI). Ketogenic medium chain triglycerides (kMCTs) could improve cognition in MCI by providing the brain with more fuel.
Methods: Fifty-two subjects with MCI were blindly randomized to 30 g/day of kMCT or matching placebo. Brain ketone and glucose metabolism (quantified by positron emission tomography; primary outcome) and cognitive performance (secondary outcome) were assessed at baseline and 6 months later.
Results: Brain ketone metabolism increased by 230% for subjects on the kMCT (P ,.001) whereas brain glucose uptake remained unchanged.
Measures of episodic memory, language, executive function, and processing speed improved on the kMCT versus baseline. Increased brain ketone uptake was positively related to several cognitive measures. Seventy-five percent of participants completed the intervention.
Discussion:A dose of 30 g/day of kMCT taken for 6 months bypasses a significant part of the brain glucose deficit and improves several cognitive outcomes in MCI.
2019 the Alzheimer’s Association. Published by Elsevier Inc. All rights reserved.
My comments: Providing a daily ketogenic drink seems to have been easy to implement and have a worthwhile positive effect on brain function in patients with early dementia. I would welcome more studies and information on how such drinks could be made commercially available out with the research setting.
Purpose: The ketogenic diet is a low-carbohydrate, moderate protein, high-fat diet that has emerged as a potential treatment for autism spectrum disorder.
Autism spectrum disorder is a neurodevelopmental disorder of social communication, and restricted, repetitive behaviors and interests in need of novel therapies.
An open-label clinical trial was done in Honolulu, Hawaii to test a modified ketogenic diet for improvement of core clinical impairments in children with ASD.
Intervention: A modified ketogenic gluten-free diet regimen with supplemental MCT was completed in 15 children ages 2 to 17 years for 3 months. Clinical (ADOS-2, CARS-2) and biochemical measures were performed at baseline and 3-months on the ketogenic diet.
Main outcome: Children administered a modified ketogenic gluten-free diet with supplemental MCT significantly improved core autism features assessed from the ADOS-2 after 3 months on diet (P = 0.006). No significant difference was observed in restricted and repetitive behavior score (P = 0.125) after 3 months on the diet protocol. Substantial improvement (> 30% decrease ADOS-2 total score) was observed in six participants, moderate improvement (> 3 units) in two participants, and minor/no improvement in seven participants. Ten participants assessed at a six-month time point sustained improvement in total ADOS-2 and social affect subdomain scores comparing baseline and 6 months (P = 0.019; P = 0.023), but no significant improvement in restricted and repetitive behavior scores were noted (P = 0.197). Significant improvements in CARS-2 items after 3 months of the modified ketogenic protocol were observed in imitation, body use, and fear or nervousness (P = 0.031, P = 0.008, P = 0.039). The percent change on ADOS-2 score from baseline to 3 months was associated with baseline high-density lipoprotein levels (ρ = −0.67, P = 0.007) and albumin levels (ρ = −0.60, P = 0.019). Moreover, the percent change from baseline to 3 months in ADOS-2 scores was significantly associated with percent change in high-density lipoprotein levels (ρ = 0.54, P = 0.049) and albumin levels (ρ = 0.67, P = 0.010).
Conclusions: A modified gluten-free ketogenic diet with supplemental MCT is a potentially beneficial treatment option to improve the core features of autism spectrum disorder and warrants further investigation.
My comment: Looking after a child with autism is very challenging. As the ketogenic diet shows promise and has a good track record for health outcomes over many years it may be worth a trial for parents or for those children living in institutional settings. If a child is also on insulin for type one diabetes careful reduction and adjustment of insulin doses will be required usually with professional help.
PHC have just released the new Real Food Healthy Lifestyle course.
It is an online course led by Liz LePlan, the PHC Ambassador Co-ordinator.
It comprises eight recorded sessions and takes people through the low carbohydrate approach. You can find it here. https://phcuk.org/support/
There is also a new Facebook group to support our work in Scotland and to try and reach out to more like-minded souls and help people who want to improve their health. We would really like you to join the group and share your own success stories and tips. Please also invite your friends and any healthcare practitioners that you know. https://www.facebook.com/groups/lowcarbrealfoodphcscotland
If you would like to watch a replay of the main event that the PHC runs each year, the Annual Conference then it is now available on YouTube.
This year the conference coincided with the 75 year anniversary of the NHS and had the theme ‘Fixing the NHS – one person at a time’.
A study published in BMJ Open reported on the analysis of 29 patient trials who were placed in group appointments in their General Practice. The participants had the same conditions as other group members.
These appointments have been seen as a way to make patient education and care more efficient. Given the constraints that Primary Care faces regarding health care professionals, this is perfectly reasonable. Group therapy, at least in theory, also allows patients to learn from each other and to support each other.
Unfortunately the outcomes were not any better for the group appointment attendees, except for lower diastolic blood pressure. There were no other statistically relevant changes. In addition, there was no difference in the use of medical services.
What can patients do to help ensure a good consultation with their GP or specialist doctor?
This was the aim of a diabetes support group. They brainstormed what they wanted to achieve and then discussed the way to get this.
The first step is preparation for your appointment.
What is the point of the consultation? Is it a first meeting, a review of progress, a follow up from a previous meeting? Think, What do I want to get out of this consultation?
Have a clear understanding of your problem if possible. Rehearse what you intend to say.
If you have a complex or worrying problem you may wish take a partner or friend with you to listen so that important information is not forgotten.
Prepare a list of questions you have for the doctor. Give it to them. This way they can figure out best how to answer comprehensively on what they can answer and tell you what they can’t answer.
During the consultation
Try to sit so you can face the doctor either side on or in front of them.
Keep it simple if you can and let the doctor know you have questions to ask, and when is it a good time to ask them.
Maintain eye contact with the doctor, encourage a two way conversation and demonstrate a desire to build a working relationship with the doctor.
Briefly summarise your symptoms.
Ask clarifying questions if you have any uncertainty such as, Why do you advise me to take these medications? Ask if there are alternative treatments.
Answer questions honestly eg if you haven’t been taking your medication as prescribed.
Be positive.
What patients want in a consultation.
Patients want to feel welcomed into the consultation. They want a doctor who shows interest, care and respect for them. A sense of humour may be appropriate.
They want to have eye contact and not just have a doctor who looks at a computer.
They want to be treated in an intelligent adult to adult way. They want the doctor to listen and to have a two way exchange.
They need the doctor to have their notes and be familiar with them.
The patient’s carer also needs to be involved in the conversation.
They need TIME to allow a relevant discussion. Often more than one issue is involved. Test results need to be explained and some patients will want specific information other than “normal” or ” a bit low”. They want options to be discussed and involved in implementing a course of action.
Patients dislike being contradicted over their experience and treatment history. They want their doctor to be frank when the doctor doesn’t know something. They welcome referral or a doctor speaking to someone with more expertise when necessary.
Some patients are very keen to have copies of letters and summaries of the discussion and action plans.
My comment:This patient group has a good structure of the ideal consultation and is similar to the sort of thing that doctors also want. In my experience there are often impediments achieving this. Such things are lack of scheduled time, interruptions, lack of continuity of doctor-patient relationships, difficulty getting notes and getting computers to work. It also helps if patients are focussed on one or at most two main issues and don’t bring a shopping list of everything that bothers them. It is helpful to involve the team of health care professionals so that things that concern eg a podiatrist or a pharmacist can be dealt with separately to the GP or consultant.




 1. In a medium mixing bowl, combine the ground cinnamon, 2 tsp. cumin, 1 tsp. coriander, flour, ½ tsp. salt, and ¼ tsp. pepper. Toss the lamb pieces with the spice mixture to coat.
1. In a medium mixing bowl, combine the ground cinnamon, 2 tsp. cumin, 1 tsp. coriander, flour, ½ tsp. salt, and ¼ tsp. pepper. Toss the lamb pieces with the spice mixture to coat.






